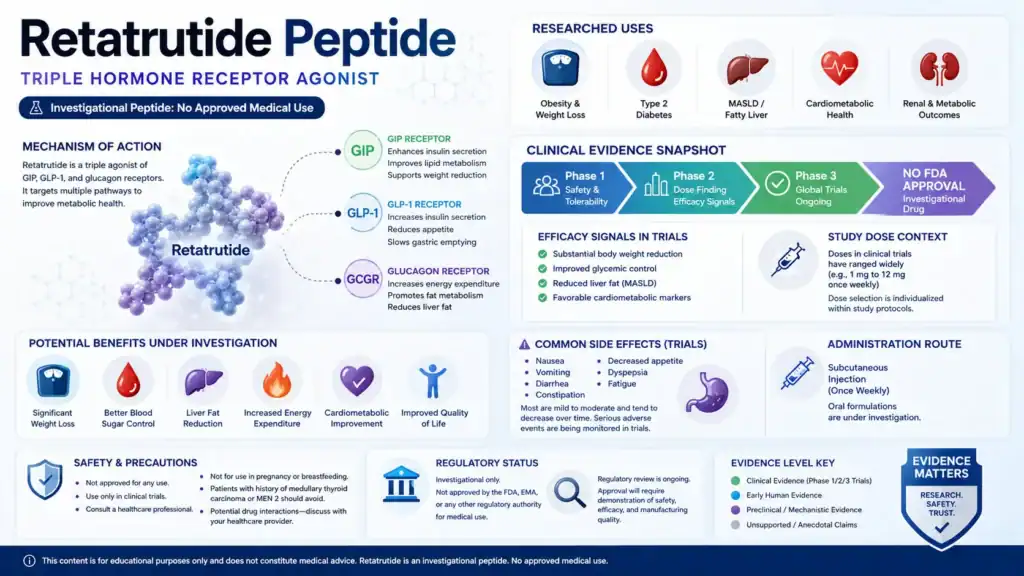
Retatrutide peptide is an investigational incretin-based metabolic drug being studied for obesity, type 2 diabetes, and related cardiometabolic conditions. Retatrutide, also known as LY3437943, is a peptide-class triple agonist that activates the GIP, GLP-1, and glucagon receptors, but it is not currently FDA-approved for any indication and is not available as an approved prescription product 1, 2, 3. This article is educational and does not provide personal medical advice, dosing instructions, or sourcing guidance.
- Retatrutide is a synthetic peptide and investigational triple hormone receptor agonist targeting GIP, GLP-1, and glucagon receptors [1], [2].
- Retatrutide is studied mainly for obesity, type 2 diabetes, metabolic dysfunction-associated steatotic liver disease, and cardiometabolic risk markers [2], 4, 5, 6.
- Human evidence includes phase 1, phase 2, and phase 3 clinical trial data, but approval decisions still depend on regulator review [2], 7.
- The strongest reported weight-loss data so far come from Lilly’s 2026 TRIUMPH-1 phase 3 topline results and earlier phase 2 obesity data [4], [7].
- Reported side effects are mainly gastrointestinal, including nausea, diarrhea, vomiting, and constipation, with dose escalation affecting tolerability [5], 8, 9.
- Retatrutide dosage information should be interpreted only as clinical-trial context, not as personal dosing guidance [4], [5], [7], [9].
- FDA states that retatrutide cannot be used in compounding under federal law and has not been found safe and effective for any condition [3].
Fast Answer: What Readers Should Know About Retatrutide
Retatrutide peptide is an investigational once-weekly triple hormone receptor agonist that activates GIP, GLP-1, and glucagon receptors and is being studied for obesity, type 2 diabetes, and related metabolic conditions [1], [2]. Clinical trials have reported large reductions in body weight and improvements in glycemic and liver-fat measures, but retatrutide remains unapproved and its long-term safety profile is still being evaluated [4], [6], [7], [8]. FDA also warns against unapproved retatrutide products and retatrutide compounding [3].
Phase 3 Development and Current Evidence Level
Retatrutide is in phase 3 development for several metabolic indications, including obesity and type 2 diabetes, while published phase 2 trials and 2026 phase 3 reports provide the main current human evidence [2], [7], [8]. The evidence is clinically meaningful but not the same as an approved-label indication.
What Retatrutide Is Not Yet Proven to Do
Retatrutide is not yet proven through regulatory approval to safely and effectively treat obesity, diabetes, liver disease, osteoarthritis, sleep apnea, kidney disease, or cardiovascular disease in routine practice [2], [3]. Online claims that describe retatrutide as available, approved, or equivalent to a marketed medicine should be treated cautiously.
Evidence basis note: This page draws from regulator statements, official trial records, peer-reviewed clinical studies, drug-development reports, and scientific databases. Claims that lack reliable clinical or regulatory support are treated as preliminary, investigational, or unverified.
What Is the Retatrutide Peptide?
Retatrutide is an investigational peptide drug candidate designed as one molecule with agonist activity at three metabolic hormone receptors: GIPR, GLP-1R, and GCGR [1], [2]. It is being developed by Eli Lilly as LY3437943 and is not an approved medication [2], [3].
Peptide Classification and Investigational Drug Context
Retatrutide is classified as a peptide and a triple peptidic agonist, with lipidation and amino-acid modifications intended to support pharmacokinetics compatible with once-weekly injection [1]. The term “GLP-3” is sometimes used online, but Lilly states that “triple agonist” is the more accurate pharmacologic description [2].
Why Retatrutide Is Studied for Obesity and Type 2 Diabetes
Retatrutide is studied in obesity and type 2 diabetes because GLP-1, GIP, and glucagon signaling each influence appetite, insulin secretion, glucose regulation, body weight, or energy metabolism [1], [5], 10. Its design attempts to combine calorie-intake reduction with broader metabolic effects, although clinical outcomes must be judged from trial data rather than mechanism alone [10].
Key Receptor Targets: GIP, GLP-1, and Glucagon
Retatrutide activates the glucose-dependent insulinotropic polypeptide receptor, glucagon-like peptide-1 receptor, and glucagon receptor [1], [2]. GLP-1 receptor agonism is associated with glucose-dependent insulin secretion, reduced glucagon secretion, slowed gastric emptying, and appetite effects, while glucagon receptor activity may influence energy expenditure and lipid metabolism [10], 11.
How Does Retatrutide Peptide Work?
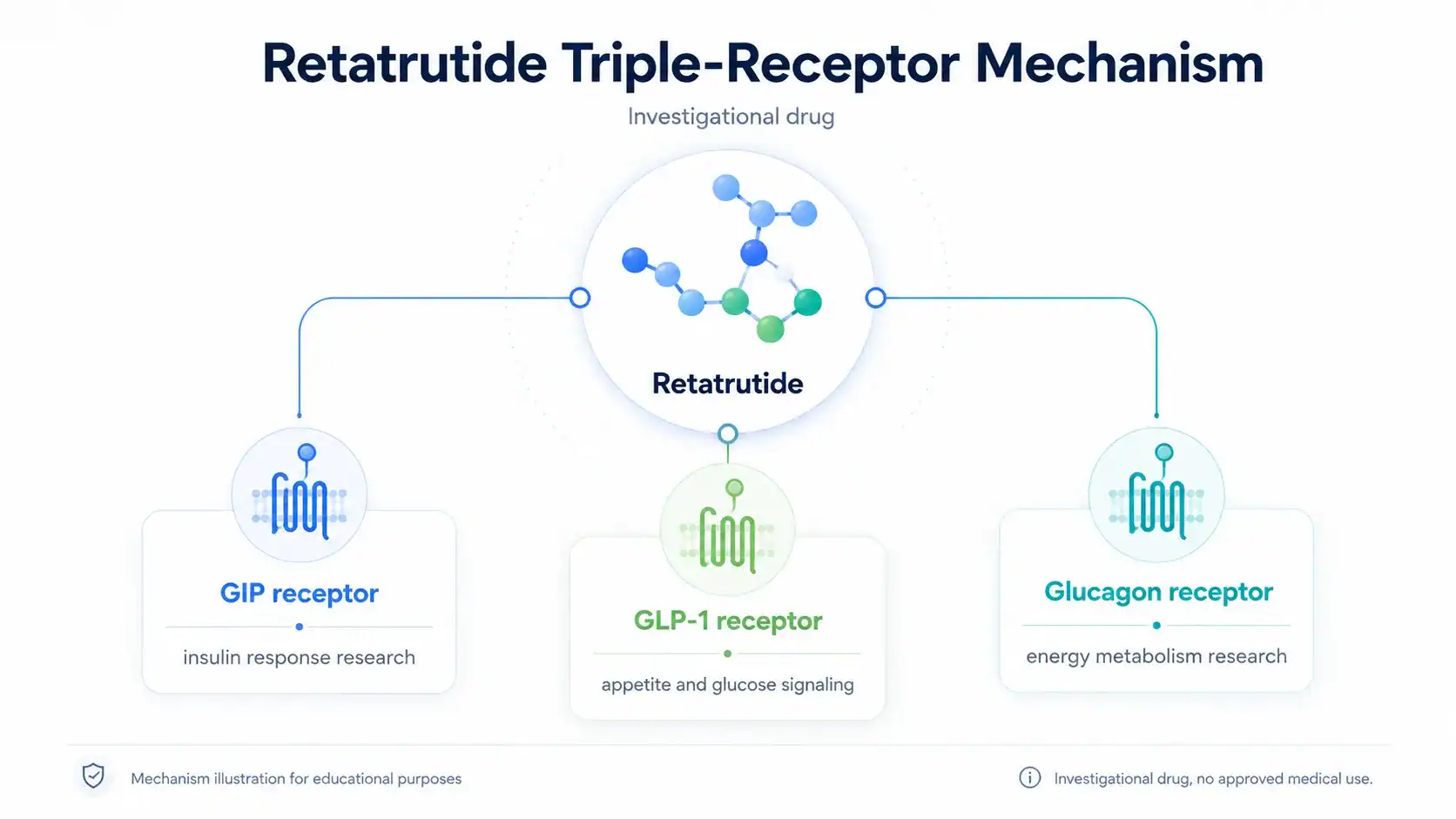
Retatrutide peptide works by activating three hormone receptor systems involved in glucose control, appetite, and energy balance [1], [2]. The proposed mechanism is biologically plausible, but clinical value depends on trial outcomes, safety data, and regulatory review rather than receptor activity alone [4], [5], [7].
GLP-1 Receptor Activity, Appetite, and Satiety
GLP-1 receptor activation can increase glucose-dependent insulin release, reduce glucagon secretion, slow gastric emptying, and influence central appetite pathways [11]. These mechanisms help explain why GLP-1 receptor agonists are used in approved therapies for type 2 diabetes or weight management, depending on product and jurisdiction 12, 13.
GIP Signaling, Insulin Response, and Metabolic Effects
GIP receptor activation is part of incretin physiology and can contribute to insulin secretion after meals, which is relevant to type 2 diabetes research [1], [10]. Retatrutide binds more strongly to GIPR than to the other target receptors in available pharmacology summaries, although receptor-binding strength does not directly translate into a guaranteed patient outcome [1].
Glucagon Receptor Activity and Energy Expenditure
Glucagon receptor activity is the feature that most clearly separates retatrutide from GLP-1-only and GLP-1/GIP dual agonists [1], [10]. Preclinical and translational work suggests glucagon signaling may influence energy expenditure and fat metabolism, but this pathway also requires careful safety evaluation because glucagon biology is tied to hepatic glucose production [10], [11].
Retatrutide Works as a Triple Hormone Receptor Agonist
Retatrutide is best understood as a triple hormone receptor agonist rather than simply another GLP-1 receptor agonist [1], [2]. The intended pharmacologic difference is simultaneous GIP, GLP-1, and glucagon receptor activation in one peptide-class molecule [1], [10].
Triple Agonist Versus Dual Agonist Therapy
Tirzepatide is an approved dual GIP/GLP-1 receptor agonist, while retatrutide is an investigational triple agonist that also activates the glucagon receptor [1], [13]. This difference makes retatrutide mechanistically distinct, but it does not automatically mean it is safer, better, or appropriate for any individual.
Why Mechanism Does Not Guarantee Clinical Outcomes
A mechanism can explain why researchers study a drug, but it cannot establish long-term benefit or safety by itself. Retatrutide’s mechanism must be interpreted alongside randomized trial results, adverse event patterns, discontinuation rates, and regulator review [4], [5], [7], [8].
Retatrutide for Weight Loss and Obesity Research
Retatrutide for weight loss is supported by human clinical trial evidence, but the evidence remains investigational rather than approved-label evidence [4], [7]. The strongest obesity signals include dose-dependent body weight reductions in phase 2 and large weight reduction in the 2026 TRIUMPH-1 phase 3 topline report [4], [7].
Adults With Obesity or Overweight in Clinical Trials
A phase 2 obesity trial evaluated once-weekly subcutaneous retatrutide in adults with obesity or overweight without type 2 diabetes and reported substantial dose-dependent reductions in body weight at 24 and 48 weeks [4]. Lilly’s 2026 TRIUMPH-1 phase 3 report described 2,339 adults with obesity or overweight, at least one weight-related comorbidity, and no diabetes [7].
Body Weight, BMI, and Average Weight Loss Outcomes
In the phase 2 obesity trial, the 8 mg and 12 mg retatrutide groups had mean body-weight reductions of 22.8% and 24.2% at 48 weeks, respectively [4]. In TRIUMPH-1, Lilly reported that participants receiving 12 mg lost an average of 70.3 lb, or 28.3%, at 80 weeks, while the 4 mg group lost 47.2 lb, or 19.0% [7].
Weight Reduction Versus Long-Term Weight Management
Weight reduction over 40 to 104 weeks does not answer every long-term weight management question. TRIUMPH-1 reported continued loss in a prespecified extension for participants with baseline BMI of at least 35, but maintenance after discontinuation, long-term adverse events, and real-world adherence remain open questions [7].
Retatrutide and Type 2 Diabetes Research
Retatrutide has been studied in people with type 2 diabetes because its receptor targets are directly relevant to glycemic control, insulin secretion, body weight, and metabolic health [5], [8]. The current evidence includes a phase 2 Lancet trial and 2026 phase 3 TRANSCEND-T2D-1 results [5], [8], [9].
Blood Sugar, Insulin Resistance, and Glycated Hemoglobin
In the 2023 phase 2 type 2 diabetes trial, retatrutide produced dose-dependent HbA1c reductions, with the 12 mg group showing a least-squares mean HbA1c change of about −2.02% at 24 weeks [5]. In TRANSCEND-T2D-1, Lilly reported mean A1C reductions of 1.7%, 2.0%, and 1.9% with 4 mg, 9 mg, and 12 mg retatrutide at 40 weeks, compared with 0.8% with placebo [9].
People With Type 2 Diabetes in Retatrutide Trials
The 2023 phase 2 diabetes trial randomized 281 participants from 42 U.S. research and health-care centers [5]. TRANSCEND-T2D-1 screened 930 participants and randomized 537 adults with type 2 diabetes and inadequate glycemic control with diet and exercise alone [8], [9].
Metabolic Health, Liver Disease, and Cardiovascular Risk
Retatrutide is being studied beyond weight loss because obesity, type 2 diabetes, liver fat, blood pressure, lipids, and inflammation often overlap in cardiometabolic disease [6], [7], [9]. These findings are promising research signals, not approved claims for treating liver or cardiovascular disease.
Metabolic Dysfunction-Associated Steatotic Liver Disease Research
A phase 2a MASLD substudy in Nature Medicine included 98 participants with metabolic dysfunction-associated steatotic liver disease and at least 10% liver fat [6]. At 24 weeks, mean relative liver-fat changes were −42.9%, −57.0%, −81.4%, and −82.4% with retatrutide 1 mg, 4 mg, 8 mg, and 12 mg, compared with +0.3% with placebo [6].
Blood Pressure, Lipids, and Cardiovascular Disease Risk Markers
TRIUMPH-1 reported improvements in waist circumference, non-HDL cholesterol, triglycerides, systolic blood pressure, and high-sensitivity C-reactive protein [7]. TRANSCEND-T2D-1 also reported improvements in non-HDL cholesterol, triglycerides, and systolic blood pressure, but these are risk markers rather than proof of fewer heart attacks, strokes, kidney outcomes, or heart failure events [9].
Clinical Trial Evidence for Retatrutide
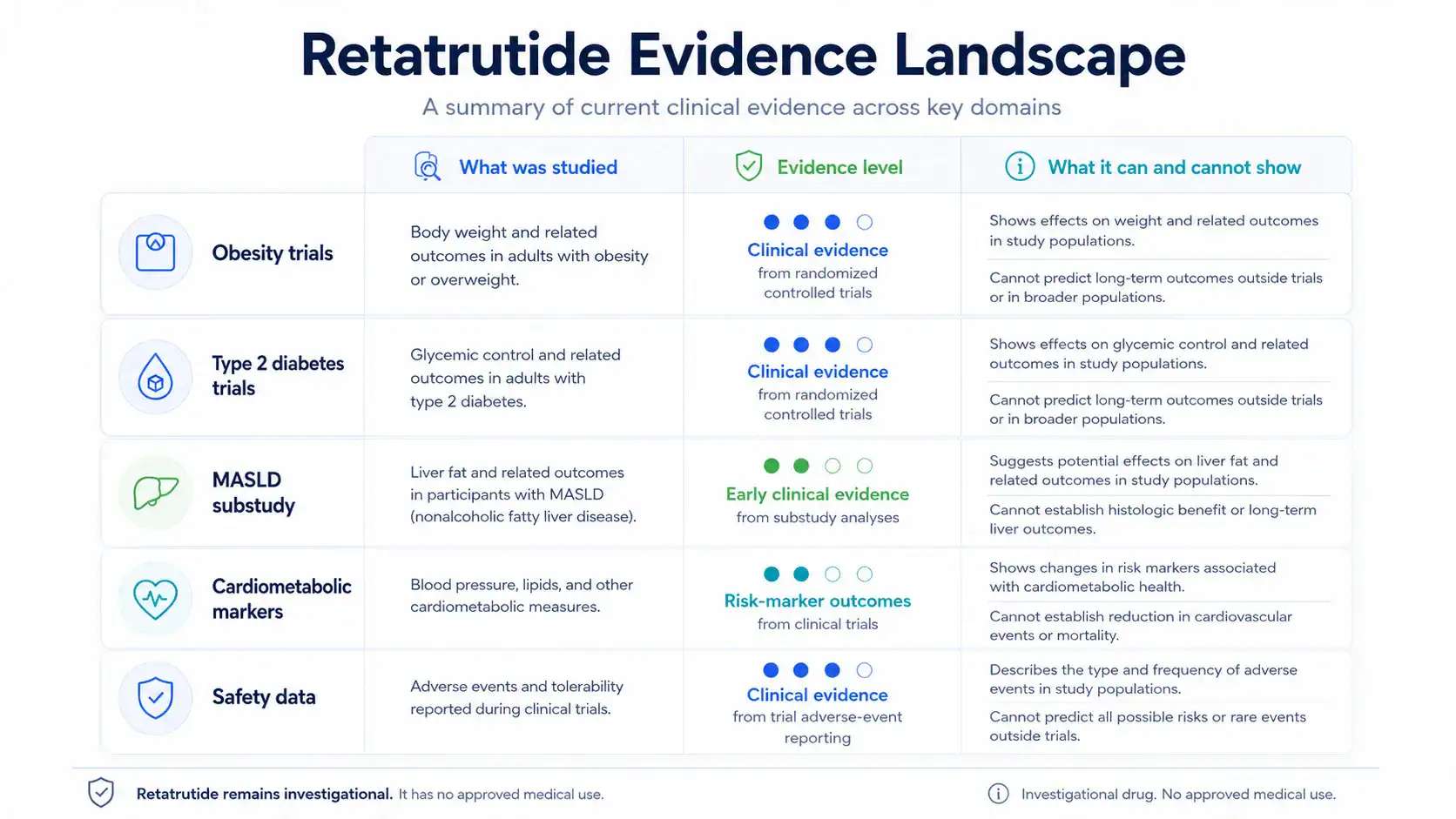
Clinical trial evidence for retatrutide is strongest for body weight reduction and glycemic outcomes, with additional early evidence for liver-fat reduction in MASLD [4], [5], [6], [7], [8]. The evidence base is still developing because long-term outcomes and regulatory review are not complete.
| Evidence Area | What Has Been Studied | Evidence Level | What It Can and Cannot Show |
|---|---|---|---|
| Obesity and body weight | Phase 2 obesity trial and TRIUMPH-1 phase 3 obesity trial data [4], [7] | Clinical evidence, investigational | Shows large study-level weight reduction; does not establish approved use or long-term real-world safety. |
| Type 2 diabetes | Phase 2 and phase 3 trials evaluating HbA1c and body weight [5], [8], [9] | Clinical evidence, investigational | Shows glycemic and weight effects in selected trial populations; does not replace approved diabetes-care guidance. |
| MASLD and liver fat | Phase 2a substudy using MRI-derived liver-fat measures [6] | Early clinical evidence | Shows liver-fat reduction signals; does not prove prevention of cirrhosis, liver events, or mortality. |
| Cardiometabolic markers | Waist circumference, lipids, systolic blood pressure, hsCRP [7], [9] | Clinical marker evidence | Suggests favorable risk-marker changes; does not prove cardiovascular outcome reduction. |
| Safety and tolerability | Adverse events, serious adverse events, discontinuation rates [5], [7], [9] | Clinical safety evidence | Identifies common events in trials; does not establish long-term population safety. |
Phase 2 Trial Findings and Dose-Response Signals
The phase 2 obesity trial reported dose-dependent body-weight reductions, with the highest-dose groups showing the largest mean losses at 48 weeks [4]. The phase 2 type 2 diabetes trial also reported dose-dependent bodyweight decreases at 36 weeks, including 16.94% in the 12 mg group versus 3.00% with placebo [5].
Phase 3 Trial Results and Pivotal Evidence
TRIUMPH-1 is a phase 3 obesity trial, and Lilly reported that 45.3% of participants receiving 12 mg achieved at least 30% body-weight reduction at 80 weeks [7]. TRANSCEND-T2D-1 is a phase 3 diabetes trial, and its 2026 data reported significant A1C and weight reductions at 40 weeks [8], [9].
Efficacy and Safety Endpoints Researchers Track
Retatrutide trials track endpoints such as percentage body-weight change, HbA1c, waist circumference, lipids, systolic blood pressure, liver fat, adverse events, serious adverse events, and treatment discontinuation [4], [5], [6], [7], [9]. Endpoint choice matters because a biomarker improvement is not the same as an approved clinical outcome.
Placebo-Controlled and Randomized Controlled Trial Design
Retatrutide’s key obesity, type 2 diabetes, and MASLD studies used randomized, double-blind, placebo-controlled designs, which help reduce bias compared with uncontrolled case reports or anecdotal reports [4], [5], [6], [8]. Even so, trial populations have eligibility criteria that may not represent every real-world patient.
Potential Benefits of Retatrutide Peptide
Potential benefits of retatrutide peptide center on obesity, body weight, glycemic control, liver-fat reduction, and cardiometabolic risk markers, but each benefit should be read by evidence level [4], [5], [6], [7], [9]. Retatrutide is not an approved treatment option at this time [2], [3].
Appetite, Satiety, and Food Intake Effects
Retatrutide’s GLP-1 and GIP-related mechanisms may influence appetite and satiety, while glucagon receptor engagement may contribute to energy metabolism [1], [10], [11]. Human trials report body-weight outcomes rather than proving every proposed appetite pathway in routine clinical use.
Reductions in Body Weight and Adipose Tissue
The best-supported potential benefit is study-level reduction in body weight among selected adults with obesity or overweight [4], [7]. In TRIUMPH-1, higher retatrutide doses produced larger average weight reductions than placebo, and waist circumference decreased in a dose-related pattern [7].
Metabolic Outcomes Beyond Weight Loss
Retatrutide studies have reported improvements in HbA1c, non-HDL cholesterol, triglycerides, systolic blood pressure, insulin resistance markers, and liver fat [5], [6], [7], [9]. These outcomes are meaningful research signals, but clinical-event outcomes such as heart attack, stroke, kidney failure, or liver decompensation need longer outcome trials.
Side Effects and Adverse Effects of Retatrutide
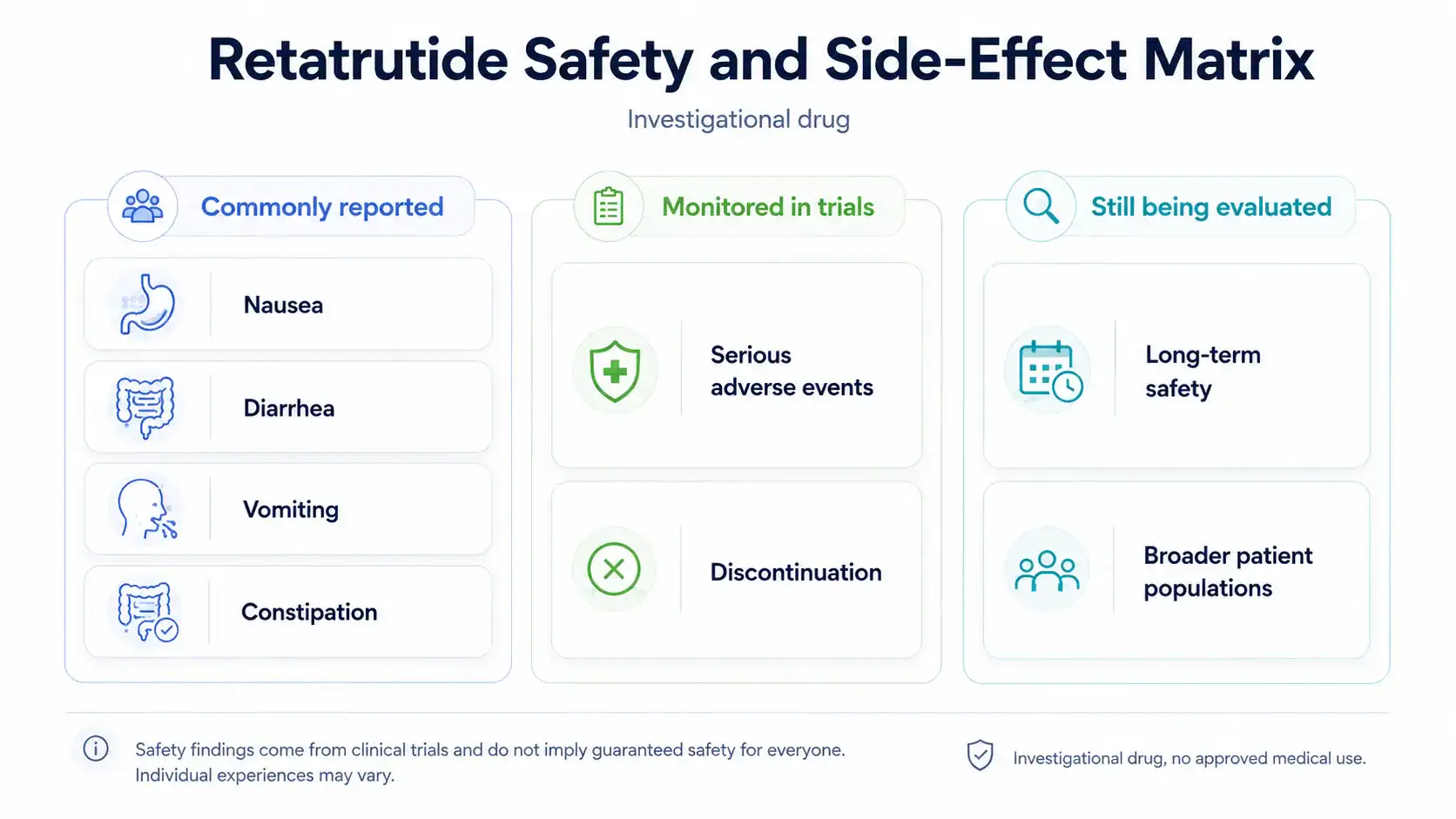
Side effects reported with retatrutide are mainly gastrointestinal, and higher doses or faster escalation can affect tolerability [5], [9]. Because retatrutide is investigational, its complete adverse-event profile is not yet defined by approved prescribing information.
Commonly Reported Gastrointestinal Side Effects
In the phase 2 type 2 diabetes trial, mild-to-moderate gastrointestinal adverse events included nausea, diarrhea, vomiting, and constipation; these events were reported in 35% of retatrutide-treated participants overall, compared with 13% with placebo [5]. In TRANSCEND-T2D-1, Lilly reported nausea, diarrhea, and vomiting as the most common adverse events [9].
Potential Side Effects at 4 mg, 9 mg, and 12 mg
TRANSCEND-T2D-1 reported nausea in 16.4%, 19.5%, and 26.5% of participants receiving 4 mg, 9 mg, and 12 mg, respectively, compared with 3.7% with placebo [9]. Lilly also reported diarrhea in 18.7%, 26.3%, and 22.8%, and vomiting in 15.7%, 15.0%, and 17.6% across the same retatrutide dose groups [9].
Serious Adverse Events and Discontinuation Signals
In TRANSCEND-T2D-1, Lilly reported adverse-event discontinuation rates of 2.2%, 4.5%, and 5.1% with retatrutide 4 mg, 9 mg, and 12 mg, compared with 0.0% with placebo [9]. In the MASLD substudy, two retatrutide-treated participants, or 2.5%, experienced a total of three serious adverse events [6].
Safety Risks, Contraindications, and Interactions
Retatrutide’s safety risks, contraindications, and interactions are not fully defined by an FDA-approved label because retatrutide is not approved [2], [3]. For now, safety interpretation should rely on clinical trial data, related incretin-drug labeling, and clinician judgment.
Pancreas, Gallbladder, Kidney, and Gastrointestinal Safety Questions
Approved GLP-1 and GLP-1/GIP therapies include warnings or precautions related to issues such as pancreatitis, gallbladder disease, acute kidney injury, severe gastrointestinal reactions, and hypersensitivity, depending on product labeling [12], [13]. Retatrutide cannot be assumed to have identical risks, but these are reasonable safety domains for clinicians and regulators to evaluate.
Diabetes Medications, Hypoglycemia Risk, and Hyperglycemia Context
Retatrutide trials in type 2 diabetes evaluate HbA1c and body weight in defined study populations, but real-world interaction questions may differ when patients use insulin, sulfonylureas, SGLT2 inhibitors, or other antihyperglycemic drugs [5], [8], [9]. The phase 2 type 2 diabetes trial reported no severe hypoglycemia and no deaths, but that does not eliminate risk in broader populations [5].
Special Population Gaps: Pregnancy, Breastfeeding, and Older Adults
Pregnancy, breastfeeding, pediatric use, frailty, advanced kidney disease, severe gastrointestinal disease, and complex polypharmacy remain areas where retatrutide-specific public evidence is limited. Approved incretin labels include special-population guidance, but retatrutide does not yet have approved labeling to guide routine clinical decisions [2], [12], [13].
Retatrutide Dosage and Administration Information From Studies
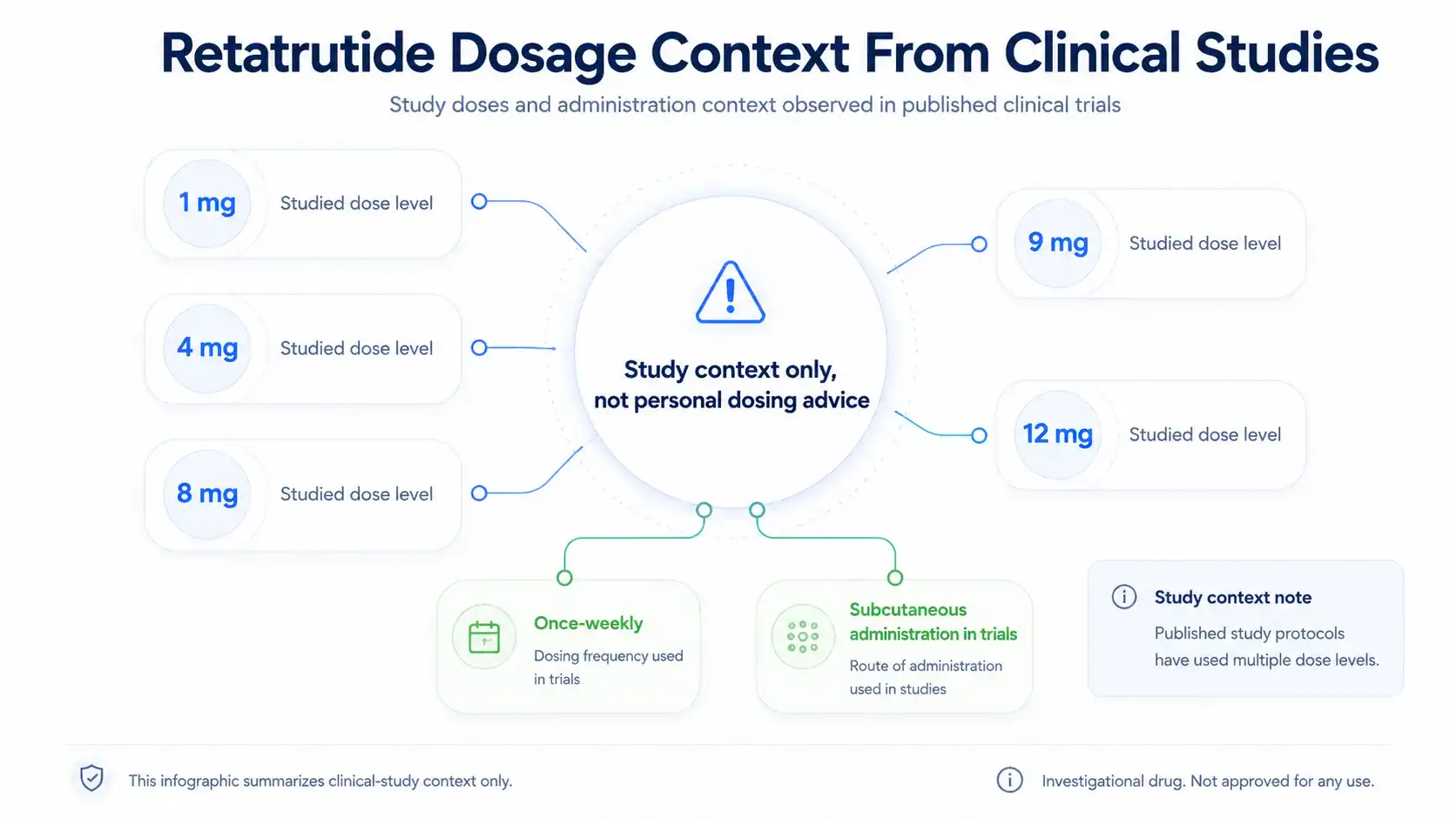
Retatrutide dosage information should be read as clinical-trial context, not as a personal dosing protocol [4], [5], [7], [9]. Published and reported studies used once-weekly subcutaneous administration under trial oversight, with dose escalation used to support tolerability [2], [5], [9].
What Dose of Retatrutide Has Been Studied?
The phase 2 type 2 diabetes trial evaluated maintenance doses including 0.5 mg, 4 mg, 8 mg, and 12 mg, with several escalation designs [5]. The phase 2 obesity trial and MASLD substudy included 1 mg, 4 mg, 8 mg, and 12 mg once-weekly subcutaneous retatrutide [4], [6]. TRIUMPH-1 evaluated 4 mg, 9 mg, and 12 mg doses [7].
Retatrutide Once Weekly and Dose Escalation Concepts
Retatrutide’s pharmacokinetic profile has been described as dose proportional with an approximately six-day half-life, supporting once-weekly dosing in clinical studies [1], [4], 14. In TRANSCEND-T2D-1, participants assigned to retatrutide started at 2 mg once weekly and escalated every four weeks to 4 mg, 9 mg, or 12 mg target doses [9].
Subcutaneous Injection, Reconstitution, and Concentration Context
Retatrutide has been administered by once-weekly subcutaneous injection in clinical trials [2], [4], [5], [9]. Because retatrutide is not an approved public-use medication and has no FDA-approved consumer vial, concentration, or reconstitution instructions, readers should not apply gray-market vial math or assume online products match the investigational drug used in trials [2], [3].
Retatrutide Compared With Semaglutide and Tirzepatide
Retatrutide differs from semaglutide and tirzepatide mainly by receptor coverage and approval status [1], [12], [13]. Semaglutide and tirzepatide have FDA-approved products for specific indications, while retatrutide remains investigational [2], [3], [12], [13].
GLP-1 Receptor Agonist Versus Triple Agonist Activity
Semaglutide is a GLP-1 receptor agonist, tirzepatide is a GIP/GLP-1 receptor agonist, and retatrutide is designed as a GIP/GLP-1/glucagon receptor agonist [1], [12], [13]. The added glucagon receptor activity is a key research distinction, not a reason to self-select one treatment over another.
Where Comparisons Are Limited Without Head-to-Head Trials
Cross-trial comparisons can be misleading because trial populations, durations, endpoints, dose escalation, background care, and missing-data methods differ. A phase 3 trial comparing retatrutide with tirzepatide in adults with obesity is listed on ClinicalTrials.gov, which should provide more direct comparison data when completed and published 15.
Regulatory Status, Evidence Gaps, and Clinician Discussion Points
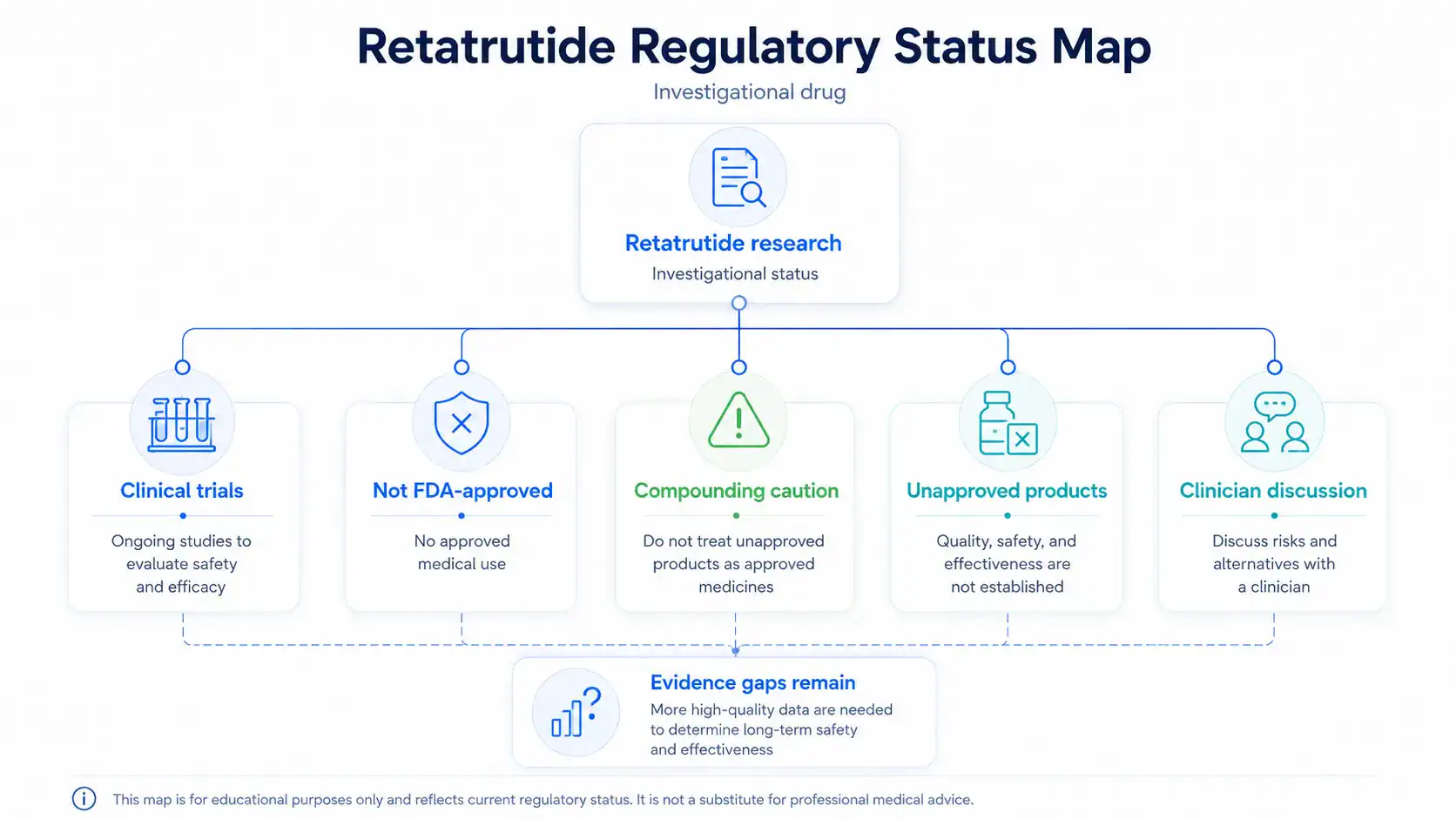
Retatrutide is investigational, not FDA-approved, and not available as an approved prescription medication [2], [3]. Regulatory status is central to interpretation because approved drugs have reviewed labeling, manufacturing standards, benefit-risk assessments, and enforceable prescribing information.
Is Retatrutide FDA-Approved or Still Investigational?
Lilly states that retatrutide is not currently approved by the FDA and is being evaluated in clinical trials [2]. FDA states that retatrutide is not a component of an FDA-approved drug and has not been found safe and effective for any condition [3].
Compounded or Unapproved Retatrutide Requires Caution
FDA states that retatrutide and cagrilintide cannot be used in compounding under federal law [3]. FDA also warns that compounded drugs are not FDA-approved and are not reviewed by FDA for safety, effectiveness, or quality before marketing [3].
What Readers Should Discuss With a Clinician
Readers considering peptide-related medical decisions should discuss evidence quality, approved alternatives, medical history, current medications, pregnancy or breastfeeding, gastrointestinal risk, pancreatitis history, gallbladder disease, kidney disease, diabetes medications, product legitimacy, and regulatory status with a licensed clinician. The safest way to interpret retatrutide peptide is through clinical-trial evidence, regulatory status, safety data, and clinician-guided decision-making, not online claims or personal protocols.
REFERENCES
- IUPHAR/BPS Guide to Pharmacology. Retatrutide ligand page. Guide to Pharmacology database. Accessed 2026.
- Eli Lilly and Company. What to know about retatrutide. Official company medical information page. Updated June 2026.
- U.S. Food and Drug Administration. FDA’s concerns with unapproved GLP-1 drugs used for weight loss. FDA drug safety and regulatory statement. 2026.
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity. New England Journal of Medicine. 2023;389:514-526. DOI: 10.1056/NEJMoa2301972.
- Rosenstock J, Frias J, Jastreboff AM, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes. The Lancet. 2023;402(10401):529-544. DOI: 10.1016/S0140-6736(23)01053-X. PMID: 37385280.
- Sanyal AJ, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease. Nature Medicine. 2024. DOI: 10.1038/s41591-024-03018-2.
- Eli Lilly and Company. Lilly’s triple agonist, retatrutide, delivered powerful weight loss in pivotal Phase 3 obesity trial. Official news release. May 21, 2026.
- Bajaj HS, Welch M, Shah P, et al. Efficacy and safety of retatrutide in people with type 2 diabetes and inadequate glycaemic control with diet and exercise. The Lancet. 2026. DOI: 10.1016/S0140-6736(26)00967-0.
- Eli Lilly and Company. Lilly’s triple agonist, retatrutide, demonstrated significant reductions in A1C and weight in first Phase 3 trial for treatment of type 2 diabetes. Official news release. March 19, 2026.
- Coskun T, Urva S, Roell WC, et al. LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss. Cell Metabolism. 2022;34(9):1234-1247.e9. DOI: 10.1016/j.cmet.2022.07.013. PMID: 35985340.
- Drucker DJ. GLP-1 physiology informs the pharmacotherapy of obesity. Molecular Metabolism. 2022;57:101351. DOI: 10.1016/j.molmet.2021.101351.
- U.S. Food and Drug Administration. Wegovy prescribing information. FDA-approved label for semaglutide injection. 2025.
- U.S. Food and Drug Administration. Zepbound prescribing information. FDA-approved label for tirzepatide injection. 2026.
- Urva S, et al. LY3437943, a novel triple GIP, GLP-1, and glucagon receptor agonist in people with type 2 diabetes. The Lancet. 2022. PMID: 36354040.
- ClinicalTrials.gov. A Study of Retatrutide Compared to Tirzepatide in Adults Who Have Obesity. NCT06662383. Clinical trial registry. 2026.
FAQs
What is retatrutide peptide and how does it work?
Retatrutide peptide is an investigational triple hormone receptor agonist that activates GIP, GLP-1, and glucagon receptors [1], [2]. This mechanism is being studied because those pathways influence appetite, blood sugar level, insulin response, body weight, and metabolism. Retatrutide is not the same as semaglutide or tirzepatide because it adds glucagon receptor activity to GIP and GLP-1 receptor signaling [1], [12], [13].
What is retatrutide being studied for?
Retatrutide is being studied for obesity, type 2 diabetes, and metabolic dysfunction-associated steatotic liver disease, also called MASLD [4], [5], [6]. Human studies have examined weight loss results, HbA1c changes, liver-fat reduction, blood pressure, lipids, and other metabolic markers. These are clinical research findings, not approved treatment claims, because retatrutide remains investigational and has not been approved for routine medical use [2], [3].
What are the commonly reported side effects of retatrutide?
Commonly reported side effects of retatrutide in clinical trials have mainly involved the gastrointestinal tract, including nausea, diarrhea, vomiting, and constipation [5], [9]. These retatrutide side effects appeared more often in some higher-dose groups and during dose escalation. Serious side effects and long-term risks are still being evaluated, so safety should be interpreted through published trial data, not online anecdotes or unapproved-product claims.
What dosage information has been reported for retatrutide?
Retatrutide dosage information comes from clinical trials, not approved prescribing instructions. Studies have evaluated once-weekly subcutaneous retatrutide at doses including 1 mg, 4 mg, 8 mg, 9 mg, and 12 mg, depending on the trial and target population [4], [5], [6], [7], [9]. These doses describe research protocols only. They should not be interpreted as a personal dosage protocol or self-use recommendation.
Is retatrutide FDA approved or legally available?
Retatrutide is not FDA approved and remains an investigational drug candidate [2], [3]. FDA has stated that retatrutide is not a component of an FDA-approved drug and cannot be used in compounding under federal law [3]. Legal status and availability can depend on jurisdiction, product type, and regulatory pathway, but unapproved retatrutide products should not be treated as equivalent to approved prescription medicines.
Who should not take retatrutide?
Who should not take retatrutide cannot be answered with an approved label because retatrutide is not yet approved [2], [3]. People with complex medical histories, pregnancy or breastfeeding considerations, diabetes medications, gastrointestinal disease, kidney disease, pancreatitis history, gallbladder concerns, or possible drug interactions should discuss risks with a licensed clinician. Off-label use, unapproved products, and self-directed treatment claims require particular caution.
Contributing Authors
The following authors are recognized for published research that helped shape the scientific and clinical context discussed in this article.
Ania M. Jastreboff
Author profile: Yale School of Medicine Profile
Ania M. Jastreboff is a clinical researcher and scientific author whose published work is directly relevant to the obesity and incretin-based clinical evidence discussed in this Retatrutide peptide article. Her publications help frame the distinction between investigational retatrutide research, established GLP-1-based obesity pharmacology, and the interpretation of clinical study outcomes. Her work is especially relevant to understanding body-weight endpoints, trial design, evidence quality, and the broader clinical context of nutrient-stimulated hormone therapies.
Selected publications:
- Triple–Hormone-Receptor Agonist Retatrutide for Obesity — New England Journal of Medicine, 2023. DOI: 10.1056/NEJMoa2301972
- Tirzepatide Once Weekly for the Treatment of Obesity — New England Journal of Medicine, 2022. DOI: 10.1056/NEJMoa2206038
Julio Rosenstock
Author profile: Google Scholar
Julio Rosenstock is a clinical research author whose publications are relevant to the type 2 diabetes, incretin pharmacology, and comparative clinical studies discussed in this article. His work helps contextualize retatrutide as an investigational GIP, GLP-1, and glucagon receptor agonist while also supporting comparison with related incretin therapies. His publications are useful for interpreting clinical studies, glycemic endpoints, dose-selection context, and safety findings in metabolic drug development.
Selected publications:
- Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes — The Lancet, 2023. DOI: 10.1016/S0140-6736(23)01053-X
- Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes — New England Journal of Medicine, 2021. DOI: 10.1056/NEJMoa2107519
PUBLISHING FIELDS
- SEO Title: Retatrutide Peptide: Uses, Safety, Dosage, Research
- Meta Description: Retatrutide peptide guide covering obesity, diabetes research, side effects, trial doses, safety, and FDA investigational status.
- Suggested URL Slug:
/retatrutide-peptide - Page Type: Therapeutic Peptide Educational Article
- ArticleFormat: Therapeutic Peptide Educational Guide
- TargetPeptide: Retatrutide
- MainKeyword: retatrutide peptide
- CanonicalKeyword: Retatrutide peptide
- ExactKeywordVariant: retatrutide peptide
- AliasTerms: retatrutide; LY3437943; triple agonist; triple hormone receptor agonist; glucagon receptor agonist; GLP-1/GIP/glucagon receptor agonist
- PeptideCategory: GLP-1 / Incretin Peptide; Cardiometabolic Peptide; Investigational Peptide
- Primary Search Intent: Therapeutic informational
- Secondary Keywords: retatrutide for weight loss; retatrutide side effects; retatrutide dosage; retatrutide clinical trial; retatrutide FDA approval; retatrutide phase 3; retatrutide type 2 diabetes; retatrutide obesity research; retatrutide vs tirzepatide; retatrutide mechanism of action; retatrutide safety; retatrutide MASLD
- Evidence Levels Covered: Clinical; early human; preclinical/mechanistic; unsupported claims; no approved medical use for retatrutide
- Excerpt: Retatrutide peptide is an investigational triple hormone receptor agonist studied for obesity, type 2 diabetes, MASLD, and metabolic outcomes. This guide reviews mechanism, clinical evidence, side effects, study-dose context, administration routes, safety concerns, and FDA regulatory status.
- Suggested Tags: Retatrutide; Incretin Peptides; GLP-1; GIP; Glucagon Receptor; Obesity Research; Type 2 Diabetes; Peptide Safety
- Featured Image Concept: Clinical evidence map showing retatrutide as an investigational GIP, GLP-1, and glucagon receptor agonist with trial evidence, safety, dosage context, and regulatory status.
- Featured Image Alt Text: Retatrutide peptide clinical evidence map showing GIP, GLP-1, glucagon receptor activity, safety, and investigational status
- Suggested Schema: Article schema only
INFOGRAPHIC BRIEFS
Infographic Brief 1
- Placement: How Does Retatrutide Peptide Work?
- Title: Retatrutide Triple-Receptor Mechanism
- Purpose: Explain how retatrutide is designed to act through GIP, GLP-1, and glucagon receptors without implying approved use or guaranteed outcomes.
- Visual Format: Mechanism of action diagram
- Key Labels: Retatrutide; GIP receptor; GLP-1 receptor; glucagon receptor; appetite signaling; insulin response; energy metabolism; investigational drug
- Suggested Layout: Center the retatrutide molecule as an abstract peptide icon with three labeled branches leading to receptor targets. Each branch should connect to a short, neutral mechanism label.
- Data or Concepts to Include: Retatrutide activates GIP, GLP-1, and glucagon receptors; GLP-1 relates to appetite and glucose-dependent insulin effects; GIP relates to insulin response; glucagon receptor activity relates to energy metabolism research.
- Visual Style: Clean clinical editorial style with simple receptor icons, muted scientific palette, and no decorative clutter.
- Compliance Restrictions: No body-transformation imagery, no injection imagery, no treatment promises, no “fat-burning” claims, no product branding.
- Alt Text: Retatrutide peptide mechanism diagram showing GIP, GLP-1, and glucagon receptor pathways
- Full AI Image Prompt: Create a clean clinical infographic titled “Retatrutide Triple-Receptor Mechanism.” Show an abstract retatrutide peptide icon in the center with three clearly labeled branches to “GIP receptor,” “GLP-1 receptor,” and “Glucagon receptor.” Under each receptor, include short neutral labels: “insulin response research,” “appetite and glucose signaling,” and “energy metabolism research.” Use a modern medical editorial style, white background, subtle blue and green accents, simple vector icons, no people, no syringes, no product packaging, no before-and-after imagery, and no guaranteed outcome language.
Infographic Brief 2
- Placement: Clinical Trial Evidence for Retatrutide
- Title: Retatrutide Evidence Landscape
- Purpose: Help readers distinguish obesity, type 2 diabetes, MASLD, cardiometabolic marker, and safety evidence by evidence level and interpretation limits.
- Visual Format: Evidence landscape table or evidence ladder
- Key Labels: Obesity trials; type 2 diabetes trials; MASLD substudy; cardiometabolic markers; safety data; clinical evidence; early clinical evidence; investigational status
- Suggested Layout: Use a vertical evidence ladder or horizontal matrix with five evidence areas and short interpretation notes beside each.
- Data or Concepts to Include: Obesity and type 2 diabetes have clinical trial evidence; MASLD has early clinical substudy evidence; cardiometabolic markers are risk-marker outcomes; safety data come from trial adverse-event reporting; retatrutide remains investigational.
- Visual Style: Editorial medical chart style with clear hierarchy, small icons, and restrained color blocks.
- Compliance Restrictions: Do not show “proven results,” before-and-after weight imagery, sales language, or approval claims. Do not include unsupported outcome claims.
- Alt Text: Retatrutide peptide evidence landscape showing obesity, type 2 diabetes, MASLD, safety, and investigational status
- Full AI Image Prompt: Create a medical editorial infographic titled “Retatrutide Evidence Landscape.” Design a clean evidence matrix with rows labeled “Obesity trials,” “Type 2 diabetes trials,” “MASLD substudy,” “Cardiometabolic markers,” and “Safety data.” Add columns labeled “What was studied,” “Evidence level,” and “What it can and cannot show.” Use concise text blocks such as “clinical evidence,” “early clinical evidence,” “risk-marker outcomes,” and “investigational status.” Use a white background, thin lines, calm blue and green accents, no people, no syringes, no product imagery, and no guaranteed outcome language.
Infographic Brief 3
- Placement: Side Effects and Adverse Effects of Retatrutide
- Title: Retatrutide Safety and Side-Effect Matrix
- Purpose: Summarize the article’s safety discussion by separating commonly reported gastrointestinal side effects, serious adverse-event monitoring, and unresolved long-term safety questions.
- Visual Format: Side-effect and safety matrix
- Key Labels: Nausea; diarrhea; vomiting; constipation; serious adverse events; discontinuation; long-term safety; investigational drug
- Suggested Layout: Three-column matrix: “Commonly reported,” “Monitored in trials,” and “Still being evaluated.” Place neutral icons beside each category.
- Data or Concepts to Include: Clinical trials reported gastrointestinal events such as nausea, diarrhea, vomiting, and constipation; trials track serious adverse events and discontinuation; long-term safety remains under evaluation because retatrutide is investigational.
- Visual Style: Clean clinical safety chart with neutral risk icons, simple typography, and no alarmist visuals.
- Compliance Restrictions: Do not imply retatrutide is safe for everyone. Do not include personal medical advice, emergency instructions, dosage instructions, or product images.
- Alt Text: Retatrutide peptide safety matrix showing gastrointestinal side effects and investigational safety questions
- Full AI Image Prompt: Create a clean clinical infographic titled “Retatrutide Safety and Side-Effect Matrix.” Show three columns labeled “Commonly reported,” “Monitored in trials,” and “Still being evaluated.” Under “Commonly reported,” include nausea, diarrhea, vomiting, and constipation. Under “Monitored in trials,” include serious adverse events and discontinuation. Under “Still being evaluated,” include long-term safety and broader patient populations. Use simple medical icons, a white background, muted blue and green accents, no syringes, no pills, no product packaging, and no language suggesting guaranteed safety.
Infographic Brief 4
- Placement: Retatrutide Dosage and Administration Information From Studies
- Title: Retatrutide Dosage Context From Clinical Studies
- Purpose: Clarify that dose information in the article refers to research protocols and studied trial doses, not personal dosing advice.
- Visual Format: Dosage context framework
- Key Labels: Study context; once-weekly; subcutaneous administration; 1 mg; 4 mg; 8 mg; 9 mg; 12 mg; not personal dosing advice
- Suggested Layout: Use a “study context only” framework with a central caution label and surrounding dose-range chips from the article.
- Data or Concepts to Include: Trials studied once-weekly subcutaneous retatrutide; published and reported study doses included 1 mg, 4 mg, 8 mg, 9 mg, and 12 mg; the article frames these as clinical-trial context, not personal instructions.
- Visual Style: Minimal clinical infographic with clear caution labeling and non-instructional layout.
- Compliance Restrictions: No step-by-step dosing, no injection tutorial, no reconstitution guide, no syringe-focused imagery, no personal protocol framing.
- Alt Text: Retatrutide peptide dosage context infographic showing study doses and once-weekly trial administration
- Full AI Image Prompt: Create a clinical infographic titled “Retatrutide Dosage Context From Clinical Studies.” Display a central label reading “Study context only, not personal dosing advice.” Around it, show simple dose chips labeled 1 mg, 4 mg, 8 mg, 9 mg, and 12 mg, plus labels for “once-weekly” and “subcutaneous administration in trials.” Use a clean white medical design with subtle blue and green accents. Do not show syringes, injection steps, reconstitution instructions, vials, product branding, or self-use protocol language.
Infographic Brief 5
- Placement: Regulatory Status, Evidence Gaps, and Clinician Discussion Points
- Title: Retatrutide Regulatory Status Map
- Purpose: Show why investigational status, FDA approval, compounding restrictions, and clinician discussion matter for interpreting retatrutide information.
- Visual Format: Regulatory and evidence-status map
- Key Labels: Investigational; not FDA-approved; clinical trials; compounding caution; unapproved products; clinician discussion; evidence gaps; approved alternatives
- Suggested Layout: Flowchart from “Retatrutide research” to “Clinical trials,” “Not FDA-approved,” “Compounding caution,” and “Clinician discussion points.”
- Data or Concepts to Include: Retatrutide is investigational; it is not FDA-approved; FDA has stated retatrutide cannot be used in compounding under federal law; unapproved products should not be treated as approved medicines; readers should discuss risks and alternatives with a clinician.
- Visual Style: Clean regulatory map with document icons, trial icons, and neutral caution markers.
- Compliance Restrictions: No sales language, no sourcing guidance, no “available now” claims, no vendor or product imagery, no personal medical instructions.
- Alt Text: Retatrutide peptide regulatory status map showing investigational status, FDA approval limits, and compounding caution
- Full AI Image Prompt: Create a clean medical regulatory infographic titled “Retatrutide Regulatory Status Map.” Use a flowchart layout beginning with “Retatrutide research” and branching to “Clinical trials,” “Not FDA-approved,” “Compounding caution,” “Unapproved products,” and “Clinician discussion.” Include a final box labeled “Evidence gaps remain.” Use professional editorial styling, white background, calm blue and green accents, document and trial icons, no people, no product packaging, no vendor imagery, no buying guidance, and no language implying availability or approved use.