
CJC-1295 No DAC peptide is a synthetic growth hormone-releasing hormone analog, often discussed under names such as CJC-1295 without DAC, CJC-1295 free base, or Modified GRF (1-29) 1 2. This educational guide explains what is known, what is uncertain, and why CJC-1295 No DAC should not be confused with the longer-acting CJC-1295 DAC form. It does not provide personalized medical advice, dosing instructions, or purchasing guidance.
- CJC-1295 No DAC is generally described as a modified GHRH analog that lacks the Drug Affinity Complex used in CJC-1295 DAC [1] [2].
- The “no DAC” distinction matters because the DAC form was designed to bind albumin and extend duration of action, while the no-DAC form is chemically distinct [2] 3.
- CJC-1295 research is tied to the growth hormone, GH, and insulin-like growth factor 1, IGF-1, axis, which is regulated by GHRH, somatostatin, ghrelin, and feedback loops 4.
- Published human evidence is limited and mostly involves CJC-1295 DAC in healthy adults, not CJC-1295 No DAC in patients with a diagnosed disease [2] 5.
- Online benefits claims around body composition, sleep, energy, fat loss, and muscle hypertrophy should be interpreted cautiously because clinical outcome evidence for CJC-1295 No DAC is not established [2].
- FDA has identified safety concerns for compounded CJC-1295, including immunogenicity concerns, peptide-related impurities, API characterization issues, increased heart rate, and systemic vasodilatory reaction 6.
- Dosage, reconstitution, and administration information in this article is educational context from labels, trials, and arithmetic principles. It is not a personal protocol.
Fast Answer
CJC-1295 No DAC peptide is a synthetic GHRH analog discussed for its relationship to pituitary growth hormone release and downstream IGF-1 signaling [1] [2] [4]. The strongest human evidence involves CJC-1295 DAC in healthy adults, while FDA found no published studies where any form of CJC-1295 was administered to subjects with a disease or condition [2] [5]. Safety and regulatory caution are central because FDA lists compounded CJC-1295 among substances that may present significant risks [6].
Evidence basis note: This page is based on official regulatory documents, FDA labeling for related approved GHRH analog therapy, PubChem compound data, ClinicalTrials.gov, and peer-reviewed literature indexed in PubMed, PMC, or major journals. Claims lacking reliable human evidence are identified as preliminary, mechanistic, or unsupported.
What Is the CJC-1295 No DAC Peptide?
CJC-1295 No DAC peptide is a modified GHRH analog that is chemically distinct from CJC-1295 DAC because it lacks the Drug Affinity Complex extension associated with albumin binding [1] [2]. FDA documents describe CJC-1295 free base and CJC-1295 DAC free base as distinct active moieties within CJC-1295-related bulk drug substances [2].
CJC-1295 No DAC, Modified GRF (1-29), and Naming Confusion
CJC-1295 No DAC is often discussed as Modified GRF (1-29), tetra-substituted GRF (1-29), or CJC-1295 without DAC [1] [2]. FDA specifically noted that inconsistent naming conventions for CJC-1295-related substances may create safety risk because patients could receive a different bulk drug substance than the prescriber intended [2].
The naming issue is not just semantic. Clinical references submitted to FDA often referred to CJC-1295 DAC even when nominations or certificates of analysis appeared to describe non-DAC CJC-1295 forms [2].
What Does “Without DAC” Mean?
“Without DAC” means the peptide lacks the Drug Affinity Complex modification used in CJC-1295 DAC [2] [3]. In the DAC version, a maleimido derivative at the C terminus was developed to support bioconjugation with albumin, which extended plasma exposure in preclinical work [3].
The no-DAC version should therefore not be interpreted through DAC pharmacokinetics unless a source specifically studied the same substance. This distinction is especially important because human half-life data from CJC-1295 DAC cannot be automatically transferred to CJC-1295 No DAC [2] [5].
Why Naming Precision Matters in Therapeutic Research
Naming precision matters because CJC-1295, CJC-1295 acetate, CJC-1295 DAC, CJC-1295 DAC acetate, and CJC-1295 DAC trifluoroacetate are not identical chemical categories [2]. FDA’s briefing document lists different molecular formulas, molecular weights, salts, and active moieties across these related substances [2].
For readers, the practical lesson is simple: evidence about “CJC-1295” must be checked for the exact form studied. A trial using CJC-1295 DAC in healthy adults does not establish the same dosing, duration, risk, or benefit profile for CJC-1295 No DAC [2] [5].
CJC-1295 With DAC vs Without DAC
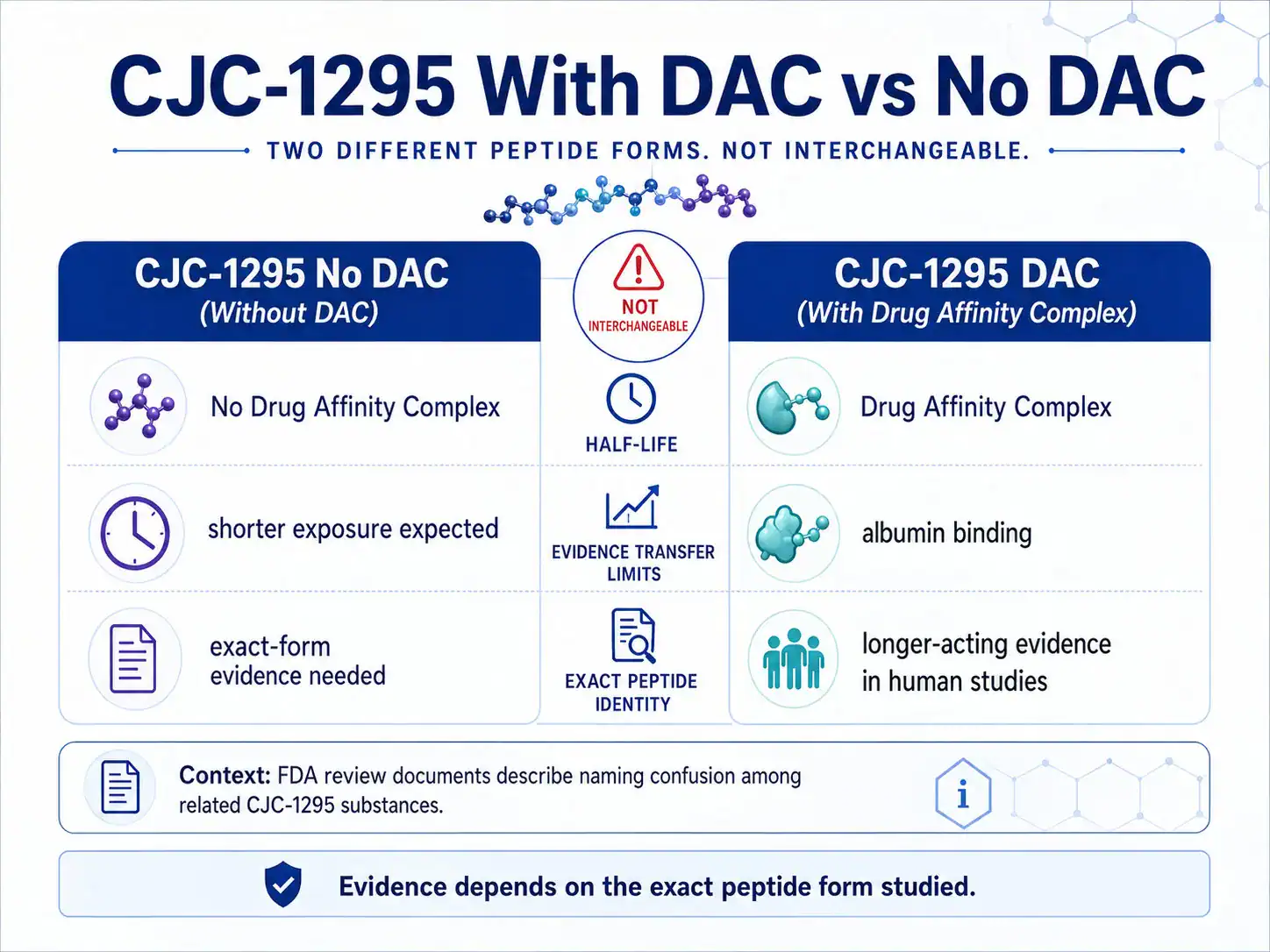
CJC-1295 with DAC and CJC-1295 without DAC differ mainly by the presence or absence of an albumin-binding Drug Affinity Complex [2] [3]. That difference changes how the peptide is expected to behave pharmacokinetically, which is why the two forms should not be treated as interchangeable.
What Is the Drug Affinity Complex?
The Drug Affinity Complex is an albumin-binding modification designed to extend the duration of a peptide in circulation [3]. Jetté and colleagues reported that CJC-1295, a tetrasubstituted hGRF(1-29) analog with a maleimido derivative of lysine at the C terminus, remained detectable in rat plasma beyond 72 hours and showed albumin-associated immunoreactivity [3].
This is the basis for the long-acting “DAC” concept. It does not describe the no-DAC form unless a source specifically states that the no-DAC form was studied.
How DAC Changes Albumin Binding and Half-Life
CJC-1295 DAC was developed to bind endogenous albumin after administration, extending the half-life of the GHRH analog [3] [5]. In healthy adults, a CJC-1295 human trial reported an estimated half-life of 5.8 to 8.1 days after subcutaneous administration, with dose-dependent increases in GH and IGF-1 [5].
CJC-1295 No DAC lacks the albumin-binding DAC modification, so the long half-life reported in that DAC trial should not be used as a no-DAC half-life estimate [2] [5].
Why the DAC Version and No DAC Version Are Not Interchangeable
The DAC version and no-DAC version are not interchangeable because chemical identity, exposure duration, and evidence base differ [2]. FDA’s review repeatedly emphasized uncertainty in which CJC-1295 form was discussed or compounded in public materials and clinical references [2].
For evidence interpretation, this means a sentence like “CJC-1295 increases IGF-1 for days” is incomplete unless it identifies the DAC form studied. The strongest published human data behind that statement involve CJC-1295 DAC, not confirmed CJC-1295 No DAC [2] [5].
How Does CJC-1295 No DAC Peptide Work?
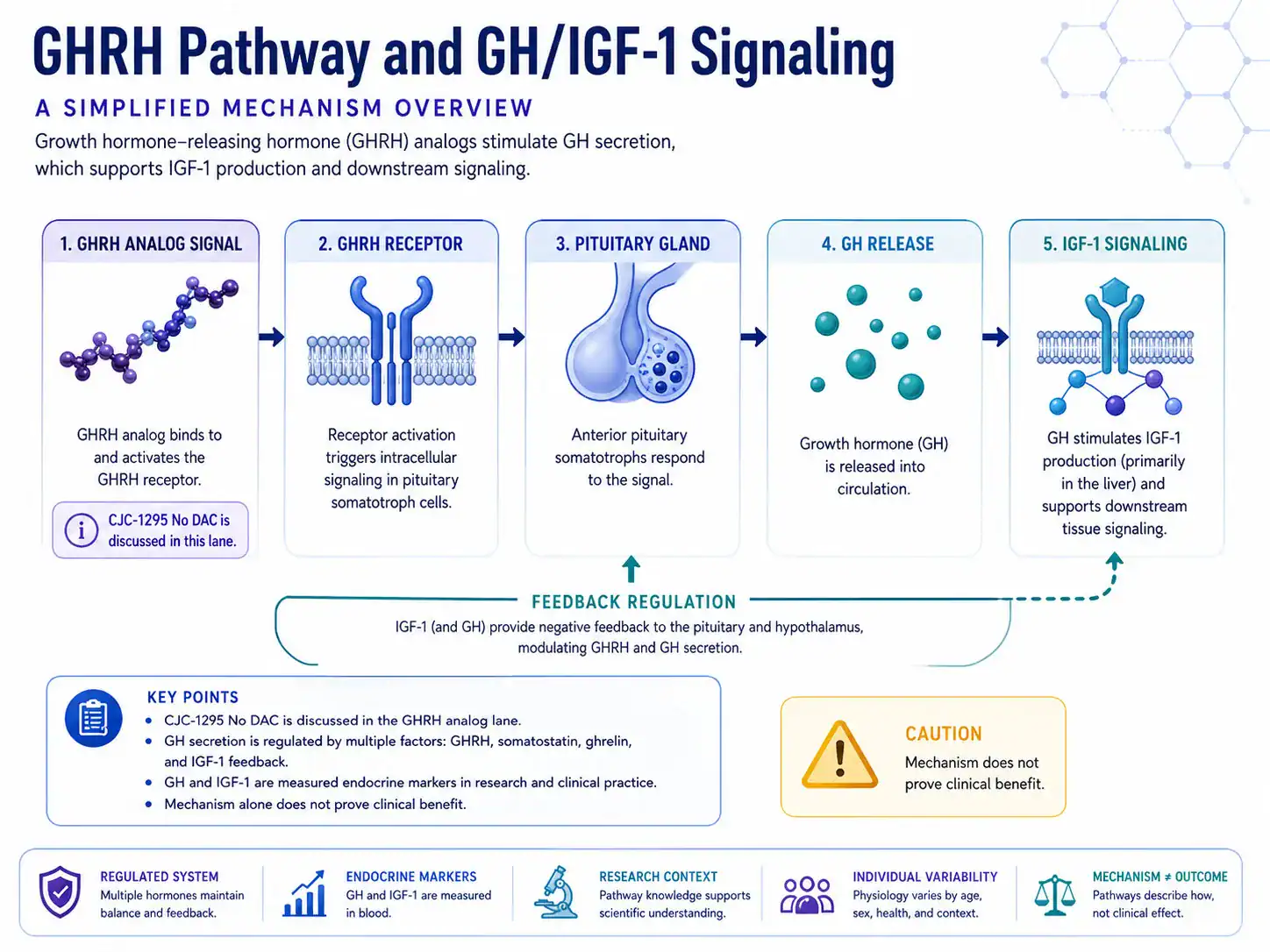
CJC-1295 No DAC peptide is proposed to work through the GHRH receptor pathway, the same biological lane used by endogenous growth hormone-releasing hormone to stimulate pituitary growth hormone secretion [4] 7. The mechanism is biologically plausible, but mechanism alone does not prove therapeutic benefit.
GHRH Receptor Activity in the Pituitary Gland
Growth hormone-releasing hormone acts on pituitary somatotroph cells to regulate growth hormone production and secretion [7]. Endotext describes GH secretion as pulsatile and regulated by GHRH stimulation, somatostatin inhibition, ghrelin signaling, and IGF-1 feedback [4].
CJC-1295 No DAC is discussed because it resembles the GHRH signaling lane. However, the reader should separate receptor-level plausibility from clinical evidence in diagnosed patients.
GH Release, Pulse Timing, and IGF-1 Signaling
GH is secreted in pulses and follows circadian patterns, with sleep and slow-wave sleep playing important roles in normal adult physiology [4]. GH acts directly and through IGF-1, and IGF-1 also feeds back at hypothalamic and pituitary levels [4].
This explains why CJC-1295 discussions often mention growth hormone levels, GH release, IGF-1, sleep, metabolism, and body composition. It does not establish that CJC-1295 No DAC improves those outcomes in clinical populations.
Why Mechanism Does Not Prove Clinical Benefit
A mechanism can explain why a peptide is studied, but clinical benefit requires human outcome data in the relevant population. FDA found three human studies in which CJC-1295 DAC was administered to healthy subjects, but no studies in which any form of CJC-1295 was administered to subjects with a disease or condition [2].
That distinction is central to this article. The growth hormone axis is real biology; broad therapeutic claims still need direct clinical evidence.
Pharmacodynamics, Half-Life, and Growth Hormone Axis Effects
CJC-1295 pharmacodynamics depend heavily on which CJC-1295 form is being discussed. The DAC form has human data showing sustained GH and IGF-1 increases, while the no-DAC form has less direct published human pharmacokinetic evidence [2] [5].
Shorter Half-Life of the Version Without DAC
CJC-1295 No DAC is expected to have shorter exposure than CJC-1295 DAC because it lacks the albumin-binding modification that was designed to extend duration [2] [3]. The precise no-DAC half-life should not be inferred from DAC trials unless the same substance and route were studied.
Older GRF(1-29) analog studies help explain the concept. In normal men, GHRH(1-29)-NH2 and a D-Ala2 analog stimulated GH release after intravenous bolus dosing, with peak responses at 15 or 30 minutes 8.
Pulsatile Secretion Versus Continuous Stimulation
Pulsatile secretion matters because normal GH physiology is not flat or constant [4]. In a healthy-male study of CJC-1295 DAC, overnight 20-minute blood sampling showed increased GH secretion with preserved pulsatility, while trough GH increased 7.5-fold and mean GH increased 46% 9.
That finding is often cited in CJC-1295 discussions, but it is still DAC evidence. CJC-1295 No DAC should be discussed separately unless no-DAC-specific data are available.
What Is CJC-1295 No DAC Peptide Used For?
CJC-1295 No DAC peptide is discussed for research and therapeutic-interest contexts involving GH release, IGF-1 signaling, and GHRH analog pharmacology [2] [4]. It is not an FDA-approved treatment for weight loss, anti-aging, muscle growth, sleep improvement, or any diagnosed disease [2] [6].
Research Contexts Involving Growth Hormone Release
The CJC-1295 research lane includes GHRH receptor activity, GH secretion, IGF-1 production, half-life modification, and peptide detection [3] [5] [9]. CJC-1295 DAC has been studied in healthy adults, and CJC-1295-related substances have been reviewed by FDA in compounding contexts [2] [5].
ClinicalTrials.gov lists a CJC-1295 study in HIV patients with visceral obesity, but the study was terminated and the exact CJC-1295 form was not provided in FDA’s discussion [2] 10.
Therapeutic Claims That Need Evidence Grading
Therapeutic claims about CJC-1295 No DAC commonly involve body composition, fat loss, muscle hypertrophy, recovery, energy, sleep, and anti-aging [2]. FDA noted online marketing for CJC-1295 around weight loss, muscle building, and anti-aging, but also concluded that available data and published literature were too limited to understand historical compounded use [2].
The strongest responsible framing is not “CJC-1295 No DAC works for these outcomes.” It is “these outcomes are discussed because of GH and IGF-1 biology, but direct no-DAC clinical evidence is limited.”
Potential Benefits of CJC-1295 No DAC Peptide
The potential benefits of CJC-1295 No DAC peptide are best understood as hypotheses linked to the GH/IGF-1 axis, not as established clinical outcomes. Human CJC-1295 DAC studies show endocrine-marker changes, while no-DAC therapeutic benefits remain insufficiently established [2] [5].
Growth Hormone and IGF-1 Related Outcomes
CJC-1295 DAC increased mean plasma GH concentrations 2-fold to 10-fold for 6 days or more and increased mean plasma IGF-1 concentrations 1.5-fold to 3-fold for 9 to 11 days after a single injection in healthy adults [5]. Those are hormone-marker outcomes, not proof of symptom improvement, disease treatment, or long-term safety.
The same trial reported that multiple CJC-1295 doses kept mean IGF-1 above baseline for up to 28 days [5]. Again, this finding applies to the studied long-acting CJC-1295 form.
Body Composition, Fat, and Lipid Metabolism Hypotheses
GH affects intermediary metabolism, protein synthesis, lipid metabolism, insulin sensitivity, and IGF-1-mediated processes [4]. That biology explains why CJC-1295 No DAC is often discussed in relation to body composition, fat, weight, energy, and muscle.
However, CJC-1295 No DAC is not the same as tesamorelin, an FDA-labeled GHRF analog indicated for reduction of excess abdominal fat in HIV-infected adults with lipodystrophy 11. EGRIFTA WR labeling also states it is not indicated for weight loss management and that long-term cardiovascular safety has not been established [11].
Sleep, Energy, and Recovery Claims
Sleep is relevant because normal GH secretion is influenced by sleep and slow-wave sleep [4]. Energy and recovery claims are more indirect because they usually rely on broad GH/IGF-1 physiology rather than direct CJC-1295 No DAC outcome trials.
Readers should treat sleep, recovery, and anti-aging claims as evidence-sensitive. The mechanism is plausible enough to explain research interest, but direct human evidence for CJC-1295 No DAC remains limited.
What Does Human Research Show About CJC-1295?
Human research shows that CJC-1295 DAC can raise GH and IGF-1 markers in healthy adults, but it does not establish CJC-1295 No DAC as a proven therapy for clinical conditions [2] [5] [9]. FDA’s review is especially important because it separates healthy-volunteer evidence from disease-treatment evidence [2].
Human Studies of CJC-1295 and Related GHRH Analogs
The main CJC-1295 human trial evidence includes two randomized, placebo-controlled, double-blind ascending-dose trials in healthy adults aged 21 to 61 years [5]. CJC-1295 or placebo was administered subcutaneously in single ascending doses and in weekly or biweekly multiple-dose schedules [5].
Another healthy-male study assessed GH pulsatility before and one week after CJC-1295 injection, with 20-minute sampling across a 12-hour overnight period [9]. A separate serum-protein profiling study reported that activation of the GH/IGF-1 axis by long-acting CJC-1295 produced serum protein profile changes in normal adults 12.
What Outcomes Have Been Measured?
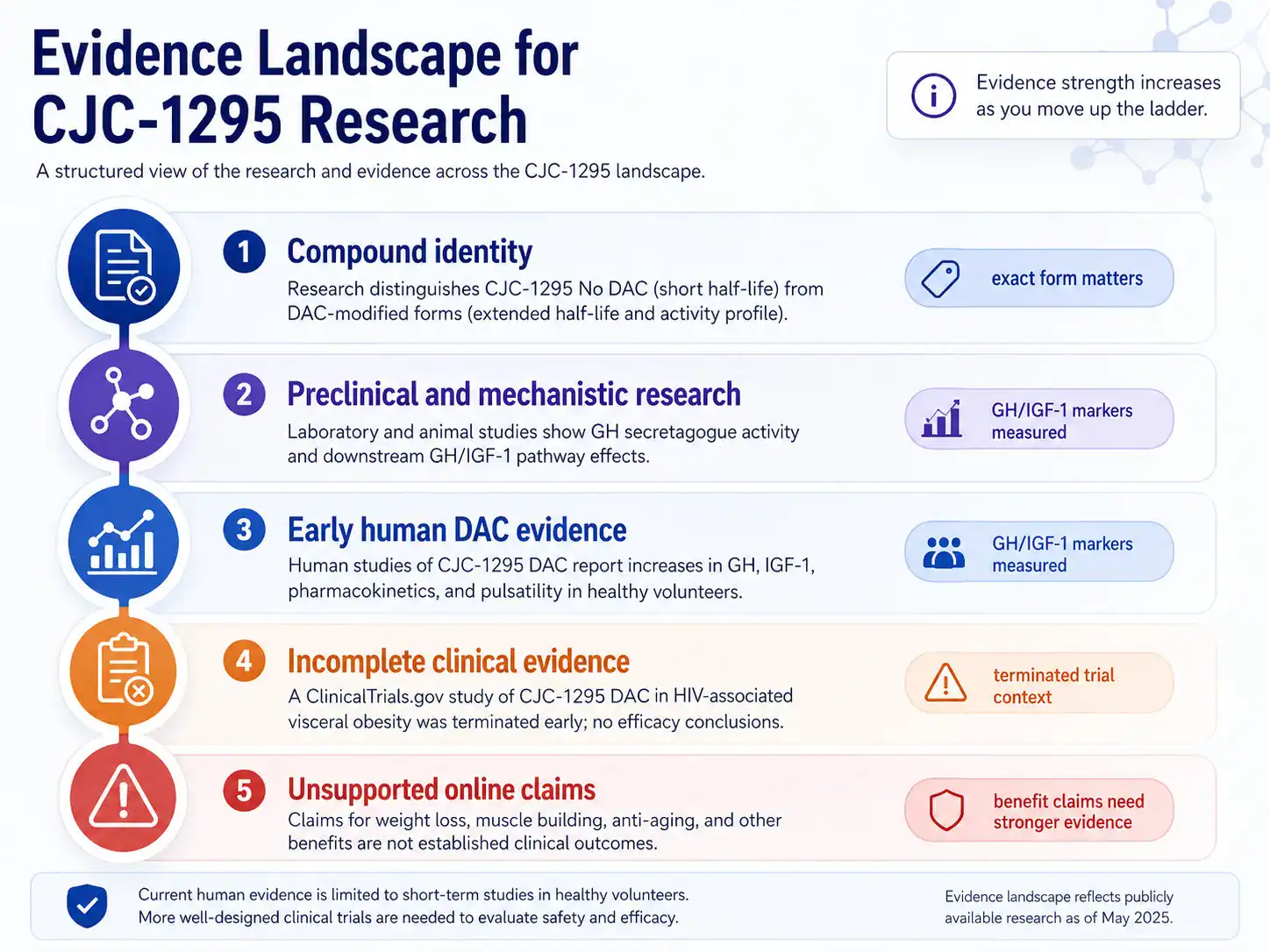
Published CJC-1295 DAC studies measured endocrine and pharmacodynamic endpoints such as GH concentrations, IGF-1 concentrations, GH pulse parameters, and protein-profile changes [5] [9] [12]. They did not establish CJC-1295 No DAC outcomes for weight loss, muscle hypertrophy, sleep quality, anti-aging, or diagnosed disease treatment [2].
| Evidence Area | What Has Been Studied | Evidence Level | What It Can and Cannot Show |
|---|---|---|---|
| CJC-1295 DAC in healthy adults | GH, IGF-1, pharmacokinetics, and tolerability in randomized trials [5] | Early human evidence | Shows endocrine-marker effects for DAC form; does not prove no-DAC therapeutic outcomes |
| GH pulsatility | Overnight GH secretion before and after CJC-1295 DAC in healthy men [9] | Early human evidence | Shows preserved pulsatility with increased trough GH; does not establish long-term clinical benefit |
| CJC-1295 in HIV visceral obesity | Terminated ClinicalTrials.gov study with form not specified [2] [10] | Incomplete clinical evidence | Cannot establish efficacy or safety because the trial was terminated |
| CJC-1295 No DAC identity | PubChem and FDA chemical-category data [1] [2] | Compound identity evidence | Helps distinguish forms; does not prove clinical effects |
| Online benefit claims | Weight loss, muscle building, anti-aging discussions noted by FDA [2] | Unsupported or anecdotal | Shows public interest; does not establish efficacy |
Why CJC-1295 With DAC Data May Not Apply to No DAC
CJC-1295 with DAC data may not apply to CJC-1295 No DAC because the DAC modification changes albumin binding and duration of exposure [2] [3]. FDA’s review noted that the active moiety in clinical references was CJC-1295 DAC even when submitted information created confusion about other CJC-1295 forms [2].
This is the key evidence limitation. The most cited human data cannot be treated as direct proof for no-DAC protocols, no-DAC safety, or no-DAC clinical outcomes.
Preclinical and Mechanistic Research on GHRH Analogs
Preclinical research supports the biological plausibility of CJC-1295-related GHRH analogs, especially receptor activation, albumin-binding design, and GH secretion. These studies are useful mechanistically, but they cannot substitute for no-DAC human safety and efficacy trials [3] 13.
Animal and Cell Models Involving GH Release
Jetté and colleagues synthesized maleimido derivatives of hGRF(1-29), tested albumin conjugates, and found GH secretion activity in cultured rat anterior pituitary cells and normal male Sprague Dawley rats [3]. The best compound, CJC-1295, showed a 4-fold increase in GH area under the curve over 2 hours compared with hGRF(1-29) in rats [3].
Alba and colleagues studied once-daily administration of long-acting CJC-1295 in a GHRH knockout mouse model, a preclinical model focused on growth and GH physiology [13]. Such models help explain pharmacology, not clinical efficacy in humans.
Receptor Signaling and Cyclic Adenosine Monophosphate
GHRH receptor signaling belongs to the pituitary somatotroph regulatory system [7]. GHRH stimulates GH synthesis and secretion through receptor-mediated endocrine signaling, while somatostatin and IGF-1 feedback help regulate the axis [4] [7].
Cyclic adenosine monophosphate is part of the broader signaling vocabulary around GHRH receptor biology, but the clinical article should avoid implying that a pathway marker equals a patient benefit. For CJC-1295 No DAC, the clinical evidence gap remains the central point.
Evidence Quality: Strong Claims, Weak Claims, and Unknowns
The evidence for CJC-1295 No DAC is strongest for compound identity and mechanistic plausibility, weaker for human endocrine effects by direct analogy, and weakest for broad therapeutic claims. The most defensible article structure separates chemical identity, DAC human data, no-DAC uncertainty, safety concerns, and online claims [1] [2] [5] [6].
Claim Strength Matrix for Therapeutic Outcomes
Strongest claims: CJC-1295 No DAC is a distinct CJC-1295-related substance without the DAC modification, and CJC-1295-related substances act in the GHRH analog lane [1] [2]. Moderate claims: CJC-1295 DAC raises GH and IGF-1 in healthy adults [5] [9]. Weak claims: CJC-1295 No DAC improves body composition, sleep, recovery, or anti-aging outcomes in humans.
This matrix matters because readers often encounter claims presented with equal confidence. The evidence does not support equal confidence.
Online Claims That Need More Evidence
FDA noted that CJC-1295 is marketed online for weight loss, muscle building, and anti-aging [2]. These claims are not the same as approved indications, controlled clinical outcome data, or validated safety guidance.
The safer editorial approach is to name the claims, explain why people connect them to GH biology, and then state that direct human evidence for CJC-1295 No DAC is not established.
What Remains Unknown About Long-Term Use?
Long-term safety, disease-specific efficacy, ideal monitoring, immunogenicity risk, and no-DAC pharmacokinetics remain insufficiently defined in reliable public evidence [2] [6]. FDA specifically states that available clinical data for CJC-1295 are limited and that compounded drugs containing CJC-1295 may raise concerns related to immunogenicity and peptide-related impurities [6].
For a GH-axis compound, uncertainty is clinically meaningful. The GH and IGF-1 pathway interacts with glucose metabolism, tissue growth signals, fluid retention, and endocrine feedback [4] [11].
Side Effects and Safety Concerns
Side effects and safety concerns for CJC-1295 No DAC should be interpreted through limited CJC-1295 data, FDA compounding concerns, and related GH-axis drug labeling. CJC-1295 No DAC does not have an FDA-approved label that defines its adverse reaction profile [2] [6].
What Side Effects Have Been Reported?
In a CJC-1295 DAC healthy-adult trial, no serious adverse reactions were reported, and the authors described tolerability as better at 30 or 60 micrograms/kg than at higher doses [5]. That finding should not be converted into a blanket safety claim for CJC-1295 No DAC.
FDA has separately identified serious adverse events associated with CJC-1295, including increased heart rate and systemic vasodilatory reaction [6]. FDA also highlights potential immunogenicity, peptide-related impurities, and API characterization issues for compounded CJC-1295 [6].
Blood Sugar, Fluid Retention, and Circulatory Considerations
GH-axis stimulation can raise safety questions around glucose intolerance, fluid retention, and tissue-growth signaling. EGRIFTA WR, the FDA-labeled tesamorelin product, warns about elevated IGF-1, fluid retention, glucose intolerance or diabetes mellitus, hypersensitivity reactions, and injection-site reactions [11].
The tesamorelin label is not a CJC-1295 No DAC label. It is still relevant as a safety-context source because both compounds are discussed in the GHRH analog and GH-release lane.
Injection-Site and Allergic Reaction Considerations
Injection-site and hypersensitivity reactions are common safety topics for injectable peptide and protein products. EGRIFTA WR labeling reports commonly observed adverse reactions including arthralgia, injection-site erythema, injection-site pruritus, pain in extremity, peripheral edema, and myalgia [11].
For compounded CJC-1295, FDA’s concerns also include immunogenicity and peptide-related impurities [6]. That makes product characterization, route, sterility, and monitoring medically relevant topics, but not a reason to provide self-use instructions.
Contraindications, Precautions, and Drug Interactions
CJC-1295 No DAC has no FDA-approved prescribing label, so contraindications and drug interactions are not established in the way they are for approved drugs. Clinician review is especially important because GH-axis activity can intersect with malignancy risk discussions, glucose metabolism, pregnancy, and other medications [2] [11].
Which Conditions Require Clinician Review?
Relevant clinician-review topics include active or prior malignancy, pituitary or hypothalamic disorders, diabetes or impaired glucose tolerance, cardiovascular symptoms, pregnancy, breastfeeding, and prior hypersensitivity reactions. These categories are informed by FDA’s CJC-1295 safety concerns and by tesamorelin labeling, not by an approved CJC-1295 No DAC label [6] [11].
EGRIFTA WR is contraindicated in patients with disruption of the hypothalamic-pituitary axis, active malignancy, known hypersensitivity to tesamorelin or excipients, and pregnancy [11]. Those contraindications should not be copied as CJC-1295 No DAC labeling, but they show why GH-axis compounds require medical context.
Interactions With Hormone Therapies and Metabolic Medications
No definitive CJC-1295 No DAC drug-interaction table exists in FDA-approved labeling because no such label exists [2] [6]. In related GH-axis labeling, EGRIFTA WR advises monitoring for potential interactions with CYP450-metabolized drugs and notes that glucocorticoid replacement requirements may change after GH stimulation [11].
Readers using corticosteroids, sex steroids, anticonvulsants, cyclosporine, diabetes medications, or hormone-related therapies should discuss the GH-axis relevance with a qualified clinician. That is a safety discussion, not a recommendation to use CJC-1295 No DAC.
Pregnancy, Breastfeeding, and Pediatric Safety Gaps
Pregnancy, breastfeeding, and pediatric safety data are not established for CJC-1295 No DAC in reliable labeling or robust clinical studies [2] [6]. EGRIFTA WR labeling contraindicates use in pregnancy and states that modifying visceral adipose tissue offers no benefit in pregnancy and could result in fetal harm [11].
Because no approved CJC-1295 No DAC label exists, the absence of defined guidance should be treated as a safety gap rather than reassurance.
CJC-1295 No DAC Dosage, Reconstitution, and Administration Context
CJC-1295 No DAC dosage information should be treated as educational context, not as a personal prescription. There is no FDA-approved CJC-1295 No DAC dosing label, and published human CJC-1295 trials mainly involve the DAC form in healthy adults [2] [5] [6].
What Dosage Information Has Been Reported or Commonly Cited?
The best-cited human CJC-1295 trial administered subcutaneous CJC-1295 or placebo in ascending single doses and in weekly or biweekly multiple-dose schedules, with dose-dependent GH and IGF-1 changes reported for the DAC form [5]. The trial’s specific reported tolerability comment favored 30 or 60 micrograms/kg compared with higher doses, but this is study context and not personal dosing advice [5].
No FDA-approved dosage exists for CJC-1295 No DAC [2] [6]. In contrast, FDA-approved EGRIFTA WR labeling for tesamorelin lists 1.28 mg subcutaneously once daily for its specific approved indication and formulation [11].
How Reconstitution Changes Concentration Calculations
Reconstitution math changes concentration by changing the amount of peptide per milliliter. The basic educational formula is: concentration equals vial amount divided by diluent volume, and volume equals reference dose divided by concentration.
For example, if a hypothetical vial contains 2 mg and is mixed to a final volume of 1 mL, the concentration is 2 mg/mL. A 0.1 mg arithmetic reference amount would correspond to 0.05 mL at that concentration. This is calculation education only, not a recommendation to prepare, inject, prescribe, or use CJC-1295 No DAC.
FDA-approved EGRIFTA WR labeling illustrates how formulation-specific reconstitution instructions can be highly specific: one 11.6 mg vial is reconstituted with 1.3 mL diluent, and the labeled dose is 1.28 mg in 0.16 mL for that product [11]. That labeled calculation applies to EGRIFTA WR, not to CJC-1295 No DAC.
Which Administration Routes Are Discussed in Medical Literature?
Published CJC-1295 DAC human trials used subcutaneous administration [5] [9]. Older GHRH(1-29) analog research in five normal men used bolus intravenous injection for GHRH(1-29)-NH2 and a D-Ala2 analog, which is useful historically but not a CJC-1295 No DAC protocol [8].
FDA-approved EGRIFTA WR is labeled for subcutaneous injection into the abdomen for its approved indication [11]. CJC-1295 No DAC has no approved administration route in FDA labeling [2] [6].
CJC-1295 No DAC and Ipamorelin Combination Claims
CJC-1295 No DAC and ipamorelin combination claims are based on the idea of using two GH-release pathways: GHRH receptor signaling and ghrelin or growth hormone secretagogue receptor signaling [4] 14. Evidence for a combination protocol should not be assumed from mechanism alone.
Why CJC-1295 Is Often Combined With Ipamorelin
Ipamorelin is described in the literature as a pentapeptide growth hormone secretagogue with GH-releasing activity in vitro and in vivo [14]. GHRH and ghrelin-related signaling can interact in normal GH physiology, which explains why combination claims appear in hormone-optimization discussions [4].
This does not establish that CJC-1295 No DAC plus ipamorelin is safe, effective, or appropriate for a given person. FDA also lists compounded ipamorelin acetate among substances raising safety concerns, including immunogenicity and peptide characterization issues [6].
Synergy Claims and Safety Questions
Synergy claims should be treated as mechanistic hypotheses unless backed by controlled clinical trials of the exact combination, route, dose, and patient population. FDA’s CJC-1295 briefing noted online CJC-1295 blends with ipamorelin and other peptides, but also stated that whether the CJC-1295 form was with or without DAC was often not provided [2].
That uncertainty is a safety problem. Combining GH-axis peptides may complicate adverse-event interpretation, glucose monitoring, IGF-1 monitoring, and causality assessment.
Regulatory Status and Clinician Discussion
CJC-1295 No DAC is not an FDA-approved peptide drug for any therapeutic indication, and FDA’s compounding review identified limited clinical data and safety concerns for CJC-1295-related substances [2] [6]. Regulatory status matters because approved and unapproved products are evaluated very differently.
Is CJC-1295 No DAC Peptide FDA-Approved?
CJC-1295 No DAC peptide is not described in FDA materials as an approved drug product with labeled indications, dosage, contraindications, or administration instructions [2] [6]. FDA’s 2024 briefing reported no approved products containing any form of CJC-1295 in multiple countries and no products authorized by the European Medicines Agency containing any form of CJC-1295 [2].
The absence of approval means there is no FDA-reviewed CJC-1295 No DAC prescribing label. Claims should therefore be judged against peer-reviewed evidence and regulatory documents, not marketing language.
Compounded Peptides, Investigational Use, and Regulatory Caution
FDA lists compounded drugs containing CJC-1295 among bulk drug substances that may present significant safety risks [6]. FDA’s concerns include immunogenicity for certain routes, peptide-related impurities, API characterization complexity, serious adverse events including increased heart rate and systemic vasodilatory reaction, and limited clinical data [6].
For athletes, there is an additional regulatory layer: the World Anti-Doping Agency lists growth hormone-releasing factors, including GHRH analogs such as CJC-1295, as prohibited substances 15. That is a sports-rule issue, separate from medical approval.
Why Purity Testing Terminology Does Not Prove Clinical Safety
Purity testing terminology such as HPLC, LC-MS, or high-resolution mass spectrometry can support identity or detection, but it does not prove clinical safety or therapeutic efficacy. Analytical research has developed detection methods for GHRH synthetic analogs including sermorelin, tesamorelin, CJC-1295, and CJC-1295 DAC 16.
FDA’s concern is broader than identity testing. The agency specifically highlights immunogenicity, peptide-related impurities, and API characterization issues in compounded CJC-1295 [6].
What Should Readers Discuss With a Clinician?
Readers considering peptide-related medical decisions should discuss CJC-1295 No DAC through the lens of evidence quality, regulatory status, medical history, medication interactions, monitoring, and approved alternatives [2] [6] [11].
A clinician-discussion checklist may include:
- Whether the exact peptide form is CJC-1295 No DAC, CJC-1295 DAC, acetate salt, or another related substance [2].
- Whether there is a diagnosed condition with approved treatment options.
- Whether GH-axis activity is appropriate to discuss given IGF-1, glucose, cardiovascular, malignancy, or pituitary history [4] [11].
- Whether current medications raise CYP450, glucocorticoid, diabetes, hormone therapy, or endocrine-monitoring concerns [11].
- Whether pregnancy, breastfeeding, pediatric use, or active malignancy makes GH-axis exposure especially risky [11].
- Whether claims being considered are backed by human trials, preclinical data, or only online reports [2].
- Whether regulatory status, compounding concerns, and adverse-event uncertainty change the risk-benefit discussion [6].
The safest way to interpret CJC-1295 No DAC peptide is through evidence quality, exact chemical identity, regulatory status, safety uncertainty, and clinician-guided decision-making. The strongest conclusions come from verified chemical and regulatory sources; broad benefit claims remain much weaker.
REFERENCES
- National Center for Biotechnology Information. CJC1295 Without DAC, PubChem Compound Summary. PubChem. Accessed 2026.
- U.S. Food and Drug Administration. FDA Briefing Document for CJC-1295 Related Bulk Drug Substances. Pharmacy Compounding Advisory Committee Meeting. 2024.
- Jetté L, Léger R, Thibaudeau K, et al. Human growth hormone-releasing factor (hGRF)1-29-albumin bioconjugates activate the GRF receptor on the anterior pituitary in rats: identification of CJC-1295 as a long-lasting GRF analog. Endocrinology. 2005. DOI: 10.1210/en.2004-1286. PMID: 15817669.
- Olarescu NC, et al. Normal Physiology of Growth Hormone in Normal Adults. Endotext, NCBI Bookshelf. Updated 2025.
- Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged Stimulation of Growth Hormone and Insulin-Like Growth Factor I Secretion by CJC-1295, a Long-Acting Analog of Growth Hormone-Releasing Hormone, in Healthy Adults. The Journal of Clinical Endocrinology & Metabolism. 2006. DOI: 10.1210/jc.2005-1536. PMID: 16352683.
- U.S. Food and Drug Administration. Certain Bulk Drug Substances for Use in Compounding that May Present Significant Safety Risks. FDA. Content current as of 2026.
- Mayo KE, Miller T, DeAlmeida V, et al. Regulation of the pituitary somatotroph cell by GHRH and its receptor. Recent Progress in Hormone Research. 2000. PMID: 11036940.
- Barron JL, Coy DH, Millar RP. Growth hormone responses to growth hormone-releasing hormone (1-29)-NH2 and a D-Ala2 analog in normal men. Peptides. 1985. DOI: 10.1016/0196-9781(85)90124-x. PMID: 2866496.
- Ionescu M, Frohman LA. Pulsatile Secretion of Growth Hormone Persists during Continuous Stimulation by CJC-1295, a Long-Acting GH-Releasing Hormone Analog. The Journal of Clinical Endocrinology & Metabolism. 2006. DOI: 10.1210/jc.2006-1702. PMID: 17018654.
- ClinicalTrials.gov. A Study to Evaluate CJC 1295 in HIV Patients With Visceral Obesity. NCT00267527. Registered 2006.
- U.S. Food and Drug Administration. EGRIFTA WR, tesamorelin for injection, Full Prescribing Information. FDA label. Revised 2025.
- Sackmann-Sala L, Ding J, Frohman LA, et al. Activation of the GH/IGF-1 axis by CJC-1295, a long acting GHRH analog, results in serum protein profile changes in normal adult subjects. Growth Hormone & IGF Research. 2009. DOI: 10.1016/j.ghir.2009.03.001. PMID: 19386527.
- Alba M, Salvatori R. Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone analog, normalizes growth in the GHRH knockout mouse. American Journal of Physiology-Endocrinology and Metabolism. 2006. DOI: 10.1152/ajpendo.00201.2006.
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology. 1998. PMID: 9849822.
- World Anti-Doping Agency. The Prohibited List. WADA. Accessed 2026.
- Memdouh S, Gavrilović I, Ng K, Cowan D, Abbate V. Advances in the detection of growth hormone releasing hormone synthetic analogs. Drug Testing and Analysis. 2021. DOI: 10.1002/dta.3183. PMID: 34665524. :::
FAQs
What does CJC-1295 No DAC peptide do?
CJC-1295 No DAC peptide is discussed for its relationship to the GHRH pathway, which is involved in pituitary growth hormone release and downstream IGF-1 signaling [4]. Most published human data involve CJC-1295 with DAC, not the no-DAC form, so claims about efficacy, muscle growth, fat loss, performance, or anti-aging should be treated as evidence-limited rather than established clinical outcomes [2] [5].
What is the difference between CJC-1295 with DAC and without DAC?
The difference between CJC-1295 with DAC and without DAC is the Drug Affinity Complex, an albumin-binding modification designed to extend the peptide’s half-life [2] [3]. CJC-1295 with DAC has published human pharmacokinetic data showing longer GH and IGF-1 effects, while CJC-1295 No DAC should not automatically be interpreted through those same data [5]. Modified GRF (1-29) is often used as a related no-DAC alias.
What are the side effects of CJC-1295 No DAC?
Side effects of CJC-1295 No DAC are not fully characterized because there is no FDA-approved CJC-1295 No DAC label defining adverse effects, contraindications, or drug interactions [2] [6]. FDA has identified safety concerns for compounded CJC-1295, including immunogenicity, peptide-related impurities, increased heart rate, and systemic vasodilatory reaction [6]. Related GH-axis labeling also highlights concerns such as glucose intolerance, fluid retention, and hypersensitivity reactions [11].
What dosage information exists for CJC-1295 No DAC?
Dosage information for CJC-1295 No DAC should be interpreted as educational context, not as a personal protocol. Published human CJC-1295 trials mainly studied the DAC form using subcutaneous dosing schedules in healthy adults [5]. There is no FDA-approved CJC-1295 No DAC dosage label [2] [6]. Any dosing, bioavailability, or administration-route discussion should be evaluated through study context, exact peptide identity, and clinician supervision.
Can CJC-1295 No DAC be combined with Ipamorelin?
CJC-1295 No DAC is often discussed with Ipamorelin because the two compounds relate to different growth hormone secretagogue pathways, but combination claims remain evidence-sensitive [4] [14]. A mechanistic rationale does not prove clinical efficacy or safety for a combined protocol. FDA has also listed compounded CJC-1295 and Ipamorelin-related substances among peptide compounding concerns, so combination use should be viewed through safety, monitoring, and regulatory caution [6].
Is CJC-1295 No DAC FDA-approved?
CJC-1295 No DAC is not FDA-approved as a peptide drug with labeled indications, dosage, contraindications, or administration instructions [2] [6]. FDA documents describe limited clinical data and safety concerns for CJC-1295-related compounded substances [6]. Legal status and clinical use can vary by jurisdiction and context, but unapproved or compounded peptide products should not be treated as equivalent to FDA-approved medicines.
Contributing Authors
The following authors are recognized for published research that helped shape the scientific and clinical context discussed in this article.
Lawrence A. Frohman
Author profile: ResearchGate
Lawrence A. Frohman authored multiple publications relevant to the clinical and pharmacology context surrounding CJC-1295, including work on growth hormone secretion, IGF-1 signaling, and the interpretation of long-acting GHRH analog evidence. His publications are especially relevant to this article because they help distinguish measured endocrine responses in human studies from broader therapeutic claims about CJC-1295 No DAC peptide. This work provides useful background for understanding pharmacodynamics, half-life, pulsatile growth hormone secretion, and the limits of extrapolating CJC-1295 DAC data to no-DAC forms.
Selected publications:
- Prolonged Stimulation of Growth Hormone and Insulin-Like Growth Factor I Secretion by CJC-1295, a Long-Acting Analog of Growth Hormone-Releasing Hormone, in Healthy Adults – The Journal of Clinical Endocrinology & Metabolism, 2006. PMID: 16352683
- Pulsatile Secretion of Growth Hormone Persists during Continuous Stimulation by CJC-1295, a Long-Acting GH-Releasing Hormone Analog – The Journal of Clinical Endocrinology & Metabolism, 2006. DOI: 10.1210/jc.2006-1702
Roberto Salvatori
Author profile: Johns Hopkins University
Roberto Salvatori’s published work is relevant to the GHRH receptor, growth hormone deficiency models, and preclinical research used to interpret CJC-1295-related pharmacology. His publications help frame the difference between mechanistic or animal-model findings and human clinical evidence. This context is important for a therapeutic informational article because CJC-1295 No DAC is often discussed through growth hormone axis biology, while evidence quality depends on the exact peptide form, study model, and clinical setting being evaluated.
Selected publications:
- Once-Daily Administration of CJC-1295, a Long-Acting Growth Hormone-Releasing Hormone Analog, Normalizes Growth in the GHRH Knockout Mouse – American Journal of Physiology-Endocrinology and Metabolism, 2006. DOI: 10.1152/ajpendo.00201.2006
- Familial Growth Hormone Deficiency and Mutations in the GHRH Receptor Gene – Vitamins and Hormones, 2004. PMID: 15196883
PUBLISHING FIELDS
- SEO Title: CJC-1295 No DAC Peptide: Uses, Risks, Research
- Meta Description: Learn what CJC-1295 No DAC peptide is, how it differs from DAC forms, what research shows, and what safety limits remain.
- Suggested URL Slug:
/cjc-1295-no-dac-peptide - Page Type: Therapeutic Peptide Educational Article
- ArticleFormat: Therapeutic Peptide Educational Guide
- TargetPeptide: CJC-1295 No DAC
- MainKeyword: cjc-1295 no dac peptide
- CanonicalKeyword: CJC-1295 No DAC peptide
- ExactKeywordVariant: cjc-1295 no dac peptide
- AliasTerms: CJC-1295 without DAC; CJC-1295 no DAC; CJC 1295; CJC; Modified GRF (1-29); GRF 1-29; CJC-1295 with DAC; CJC-1295 DAC; DAC version; DAC variant; Drug Affinity Complex; GHRH analog
- PeptideCategory: GHRH Analog
- Primary Search Intent: Therapeutic informational
- Secondary Keywords: CJC-1295 without DAC; CJC-1295 with DAC vs without DAC; CJC-1295 DAC; Modified GRF (1-29); GHRH analog; CJC-1295 side effects; CJC-1295 dosage information; CJC-1295 and Ipamorelin; CJC-1295 FDA approval; CJC-1295 half-life; growth hormone release peptide research; CJC-1295 peptide therapy
- Evidence Levels Covered: approved-label context for related tesamorelin; early human evidence for CJC-1295 DAC; preclinical evidence for GHRH analog research; unsupported or evidence-limited claims for CJC-1295 No DAC outcomes
- Excerpt: CJC-1295 No DAC is a GHRH analog discussed for growth hormone and IGF-1 signaling. This guide explains DAC vs no DAC differences, research evidence, possible benefits, side effects, dosage context, regulatory status, and key safety limitations.
- Suggested Tags: CJC-1295 No DAC; GHRH analogs; growth hormone research; peptide safety; peptide pharmacology; CJC-1295 DAC; Modified GRF (1-29); investigational peptides
- Featured Image Concept: Clinical evidence map showing CJC-1295 No DAC identity, DAC vs no DAC distinction, GH/IGF-1 pathway context, evidence strength, and safety considerations.
- Featured Image Alt Text: Clinical evidence map for CJC-1295 No DAC peptide showing DAC comparison, GH axis context, and safety evidence levels.
- Suggested Schema: Article schema only.
INFOGRAPHIC BRIEFS
Infographic Brief 1
- Placement: After
## CJC-1295 With DAC vs Without DAC - Title: CJC-1295 With DAC vs No DAC
- Purpose: Explain the central naming and pharmacology distinction between CJC-1295 DAC and CJC-1295 No DAC so readers do not interpret the two forms as interchangeable.
- Visual Format: Side-by-side comparison chart
- Key Labels: CJC-1295 No DAC; CJC-1295 DAC; Drug Affinity Complex; albumin binding; half-life; evidence transfer limits; exact peptide identity
- Suggested Layout: Two vertical columns compare “Without DAC” and “With DAC.” A center divider highlights “not interchangeable.” A small bottom note box says “Evidence depends on the exact form studied.”
- Data or Concepts to Include: DAC form uses a Drug Affinity Complex designed for albumin binding; CJC-1295 DAC has published human pharmacokinetic evidence; CJC-1295 No DAC should not automatically be interpreted through DAC data; FDA documents describe naming confusion among related CJC-1295 substances.
- Visual Style: Clean clinical editorial style, simple vector icons, restrained colors, no product packaging, no decorative clutter.
- Compliance Restrictions: No injection imagery, no dosing visuals, no vial preparation, no product sales imagery, no personal-use protocol language, no claims that one form is better for an individual.
- Alt Text: Comparison chart explaining CJC-1295 No DAC peptide versus CJC-1295 DAC, including Drug Affinity Complex, albumin binding, half-life, and evidence limits.
- Full AI Image Prompt: Create a clean clinical infographic titled “CJC-1295 With DAC vs No DAC.” Use a two-column comparison layout. Left column: “CJC-1295 No DAC” with labels “No Drug Affinity Complex,” “shorter exposure expected,” “exact-form evidence needed.” Right column: “CJC-1295 DAC” with labels “Drug Affinity Complex,” “albumin binding,” “longer-acting evidence in human studies.” Add a center divider labeled “Not interchangeable.” Add a small footer note: “Evidence depends on the exact peptide form studied.” Use abstract molecule and pathway icons only. No syringes, vials, dosing marks, product packaging, before-and-after imagery, vendor branding, or personal-use instructions.
Infographic Brief 2
- Placement: After
## How Does CJC-1295 No DAC Peptide Work? - Title: GHRH Pathway and GH/IGF-1 Signaling
- Purpose: Show the proposed mechanism of action in a simplified, non-promotional way by connecting GHRH receptor activity, the pituitary gland, GH release, and IGF-1 signaling.
- Visual Format: Mechanism of action diagram
- Key Labels: GHRH analog; GHRH receptor; pituitary gland; GH release; IGF-1; feedback loops; mechanism does not prove benefit
- Suggested Layout: Left-to-right pathway: GHRH analog signal → GHRH receptor on pituitary → GH release → IGF-1 signaling. Include a feedback-loop arrow and a caution callout: “Mechanism supports research interest, not proven outcomes.”
- Data or Concepts to Include: CJC-1295 No DAC is discussed in the GHRH analog lane; GH secretion is regulated by GHRH, somatostatin, ghrelin, and IGF-1 feedback; GH and IGF-1 are measured endocrine markers; mechanism alone does not prove clinical benefit.
- Visual Style: Medical textbook-inspired, clean vector pathway, subtle clinical color palette, minimal text.
- Compliance Restrictions: No human body transformation imagery, no muscle-growth imagery, no anti-aging visuals, no performance imagery, no guaranteed benefit language, no injection or dosing elements.
- Alt Text: Mechanism diagram for CJC-1295 No DAC peptide showing GHRH receptor signaling, pituitary GH release, IGF-1 signaling, and evidence limitations.
- Full AI Image Prompt: Create a medical editorial mechanism diagram titled “GHRH Pathway and GH/IGF-1 Signaling.” Show a simplified left-to-right pathway using abstract icons: “GHRH analog signal” → “GHRH receptor” → “pituitary gland” → “GH release” → “IGF-1 signaling.” Add a curved feedback arrow labeled “feedback regulation.” Include a small caution box: “Mechanism does not prove clinical benefit.” Use clean lines, neutral clinical colors, no people, no syringes, no vials, no dosing charts, no fitness imagery, no anti-aging imagery, and no product branding.
Infographic Brief 3
- Placement: After
### What Outcomes Have Been Measured? - Title: Evidence Landscape for CJC-1295 Research
- Purpose: Convert the article’s evidence table into a scannable visual that distinguishes early human CJC-1295 DAC evidence, compound identity evidence, incomplete trial evidence, and unsupported online claims.
- Visual Format: Evidence ladder and evidence-area map
- Key Labels: compound identity; early human evidence; CJC-1295 DAC studies; terminated trial; preclinical evidence; unsupported claims; evidence gaps
- Suggested Layout: A vertical evidence ladder with tiers from “compound identity” and “preclinical/mechanistic” through “early human DAC evidence” and “incomplete clinical evidence,” ending with “unsupported claims.” Each tier includes one short example from the article.
- Data or Concepts to Include: Human DAC studies measured GH, IGF-1, pharmacokinetics, and pulsatility; a ClinicalTrials.gov HIV visceral obesity study was terminated; compound identity sources distinguish CJC-1295 No DAC from DAC forms; online claims around weight loss, muscle building, and anti-aging are not established clinical outcomes.
- Visual Style: Editorial science graphic, structured hierarchy, clear evidence labels, no sensational imagery.
- Compliance Restrictions: No guaranteed outcome language, no before-and-after visuals, no weight-loss imagery, no muscle-building imagery, no “results” imagery, no claims that early evidence proves therapeutic benefit.
- Alt Text: Evidence landscape infographic for CJC-1295 No DAC peptide showing compound identity, early human DAC evidence, preclinical research, incomplete trial evidence, and unsupported claims.
- Full AI Image Prompt: Create a clean evidence ladder infographic titled “Evidence Landscape for CJC-1295 Research.” Use five stacked tiers labeled “Compound identity,” “Preclinical and mechanistic research,” “Early human DAC evidence,” “Incomplete clinical evidence,” and “Unsupported online claims.” Add concise callouts: “exact form matters,” “GH/IGF-1 markers measured,” “terminated trial context,” and “benefit claims need stronger evidence.” Use a clinical editorial style with icons for documents, pathway nodes, study chart, and caution flag. Do not include people, bodies, syringes, vials, product labels, before-and-after images, weight-loss graphics, bodybuilding imagery, or promotional language.
Infographic Brief 4
- Placement: After
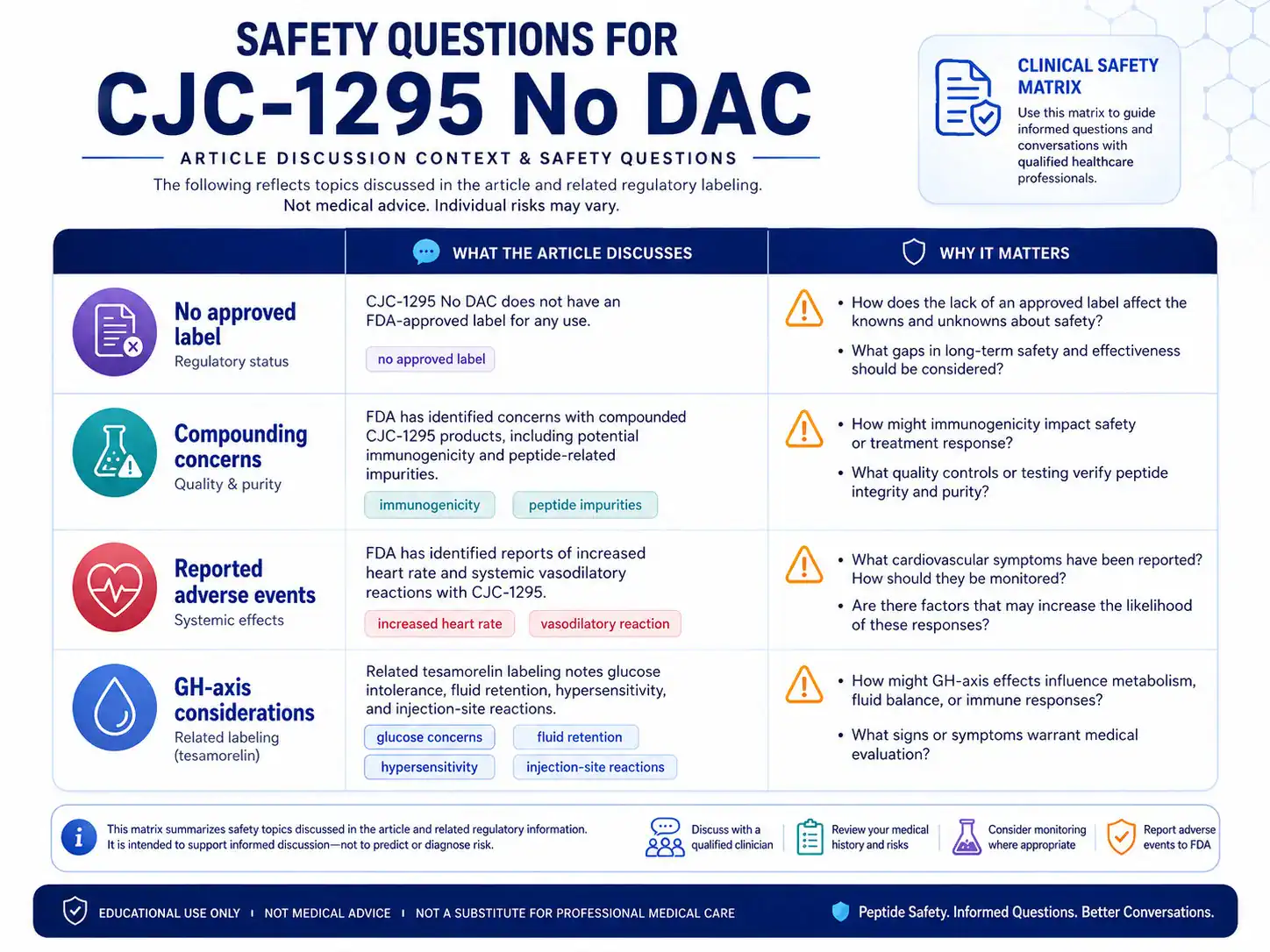
## Side Effects and Safety Concerns - Title: Safety Questions for CJC-1295 No DAC
- Purpose: Help readers understand why safety discussions should include FDA concerns, GH-axis considerations, adverse events, and the absence of an approved CJC-1295 No DAC label.
- Visual Format: Safety matrix
- Key Labels: no approved label; immunogenicity; peptide impurities; increased heart rate; vasodilatory reaction; glucose concerns; fluid retention; hypersensitivity
- Suggested Layout: Matrix with four rows: “Regulatory status,” “Compounding concerns,” “Reported adverse events,” and “GH-axis considerations.” Columns show “What the article discusses” and “Why it matters.”
- Data or Concepts to Include: No FDA-approved CJC-1295 No DAC label; FDA identified immunogenicity and peptide-related impurity concerns for compounded CJC-1295; FDA identified increased heart rate and systemic vasodilatory reaction; related tesamorelin labeling discusses glucose intolerance, fluid retention, hypersensitivity, and injection-site reactions.
- Visual Style: Clinical safety card format, clear caution icons, professional editorial look.
- Compliance Restrictions: No alarmist imagery, no emergency-room imagery, no self-injection visuals, no drug packaging, no personal risk diagnosis, no suggestion that risks apply equally to all individuals.
- Alt Text: Safety matrix for CJC-1295 No DAC peptide showing regulatory status, compounding concerns, adverse events, and GH-axis safety considerations.
- Full AI Image Prompt: Create a clinical safety matrix infographic titled “Safety Questions for CJC-1295 No DAC.” Use a four-row table with rows labeled “No approved label,” “Compounding concerns,” “Reported adverse events,” and “GH-axis considerations.” Include short labels: “immunogenicity,” “peptide impurities,” “increased heart rate,” “vasodilatory reaction,” “glucose concerns,” “fluid retention,” and “hypersensitivity.” Use subtle caution icons and clean medical editorial styling. Do not show syringes, vials, injection sites, product packaging, emergency scenes, before-and-after imagery, or personal medical instructions.
Infographic Brief 5
- Placement: After
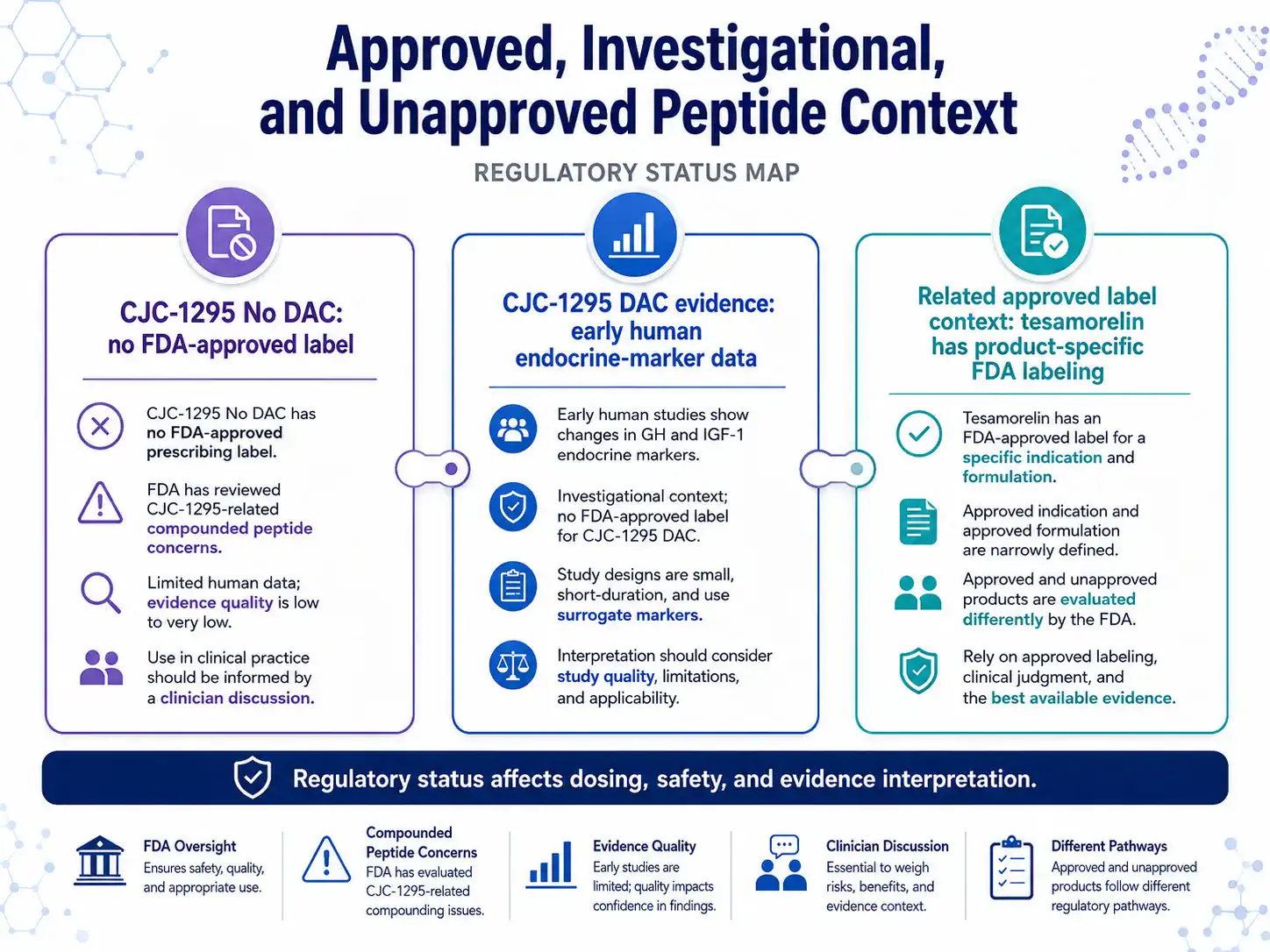
## Regulatory Status and Clinician Discussion - Title: Approved, Investigational, and Unapproved Peptide Context
- Purpose: Clarify how CJC-1295 No DAC differs from related approved-drug context and why regulatory status matters for evidence interpretation and safety.
- Visual Format: Regulatory status map
- Key Labels: CJC-1295 No DAC; not FDA-approved; compounded peptide concerns; CJC-1295 DAC evidence; tesamorelin label context; clinician discussion; evidence quality
- Suggested Layout: Three connected cards: “CJC-1295 No DAC,” “CJC-1295 DAC evidence,” and “Related approved label context.” A lower banner states “Regulatory status affects dosing, safety, and evidence interpretation.”
- Data or Concepts to Include: CJC-1295 No DAC has no FDA-approved prescribing label; FDA reviewed CJC-1295-related compounding concerns; CJC-1295 DAC has early human evidence; tesamorelin has an FDA-approved label for a specific indication and formulation; approved and unapproved products are evaluated differently.
- Visual Style: Clean policy-and-science explainer, editorial, neutral, evidence-focused.
- Compliance Restrictions: No “legal workaround” language, no buying or vendor imagery, no product promotion, no implication that unapproved products are equivalent to approved medicines, no personal-use instructions.
- Alt Text: Regulatory status map for CJC-1295 No DAC peptide showing FDA approval status, CJC-1295 DAC evidence, related tesamorelin label context, and clinician discussion points.
- Full AI Image Prompt: Create a clean regulatory status map titled “Approved, Investigational, and Unapproved Peptide Context.” Show three connected cards: “CJC-1295 No DAC: no FDA-approved label,” “CJC-1295 DAC evidence: early human endocrine-marker data,” and “Related approved label context: tesamorelin has product-specific FDA labeling.” Add a bottom banner: “Regulatory status affects dosing, safety, and evidence interpretation.” Use a professional medical editorial design, document icons, evidence icons, and neutral colors. Do not include product packaging, vendor branding, purchase language, syringes, vials, self-use instructions, or claims that unapproved peptides are safe or effective.