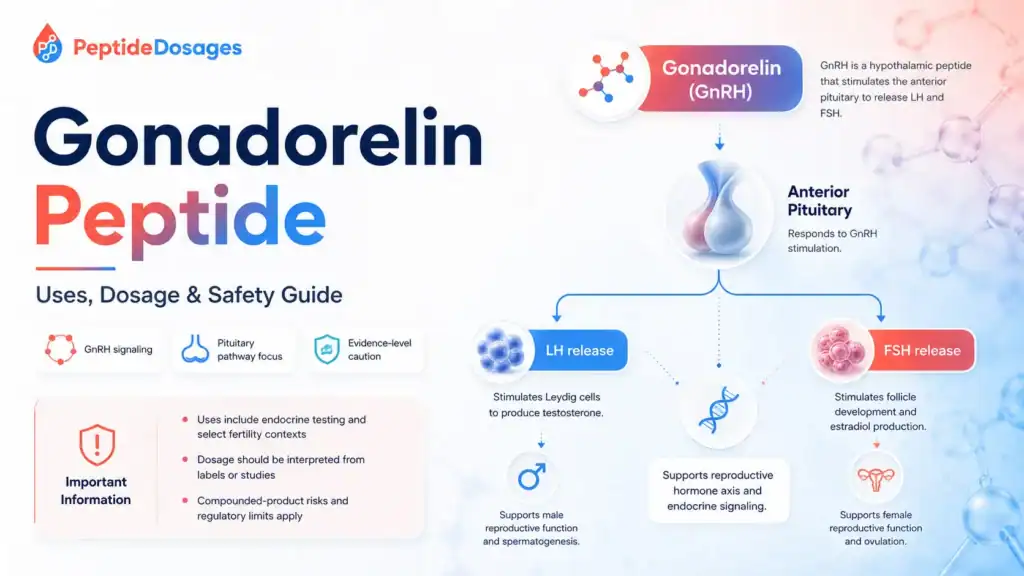
Gonadorelin peptide is a synthetic form of gonadotropin-releasing hormone, or GnRH, the hypothalamic signal that helps regulate luteinizing hormone and follicle-stimulating hormone release from the pituitary gland 1 5. This educational guide explains its mechanism, approved and studied uses, potential benefits, side effects, dosage information from labels and studies, administration routes, and regulatory status without giving personal medical advice. In the United States, a gonadorelin hydrochloride product has had FDA-approved diagnostic labeling, while compounded gonadorelin products are not FDA-approved as compounded drugs 3 13.
Quick summary
- Gonadorelin is a synthetic decapeptide that corresponds to endogenous GnRH, also called gonadotropin-releasing hormone [1] 2.
- Gonadorelin works through the GnRH receptor in the anterior pituitary, where appropriate pulsatile signaling can stimulate LH and FSH release [5] 6.
- Approved gonadorelin hydrochloride labeling has focused on diagnostic evaluation of pituitary gonadotrope function, not broad wellness or anti-aging use [3] 4.
- Human research has examined pulsatile gonadorelin therapy in selected reproductive endocrine disorders, including congenital or idiopathic hypogonadotropic hypogonadism and functional hypothalamic amenorrhea 8 11.
- The potential benefits of gonadorelin depend on the clinical context, pituitary responsiveness, reproductive goals, and whether use is diagnostic, therapeutic, investigational, or unsupported [4] [8].
- Side effects of gonadorelin reported in labeling and literature are generally interpreted in medical context and may include transient systemic symptoms or injection-site reactions; serious reactions require clinical evaluation [4].
- Dosage and administration information should be read only as approved-label or published-study context, not as a personal dosing protocol [4] [8] [11].
Fast Answer
Gonadorelin peptide is synthetic GnRH, a reproductive peptide hormone that signals the anterior pituitary to release LH and FSH when given in an appropriate physiologic pattern [1] [5]. People search for it because of pituitary testing, fertility, testosterone, HCG comparisons, and hormone therapy questions. Evidence is strongest for approved diagnostic use and selected clinician-supervised fertility contexts; it is weaker for online claims about TRT support or general hormone optimization [3] [8] [11]. Safety, dosage, and legality depend on product, indication, route, and medical supervision [4] [13].
What Is the Gonadorelin Peptide?
Gonadorelin is the synthetic medication form of GnRH, a naturally occurring hormone signal made by the hypothalamus and released in pulses to regulate the reproductive endocrine system [1] [5]. It is discussed as a therapeutic peptide because its effects connect directly to LH and FSH release, ovulation, testosterone production, and spermatogenesis, but those effects depend strongly on diagnosis and dosing pattern [5] [6].
Gonadorelin as a Synthetic GnRH Peptide Hormone
Gonadorelin is a decapeptide, meaning it contains 10 amino acid residues, and databases describe it as equivalent to the endogenous GnRH sequence with a pyroglutamyl N-terminus and amidated C-terminus [1] [2]. In plain terms, gonadorelin is a synthetic peptide hormone designed to mimic the hypothalamic GnRH signal rather than directly replacing testosterone, estrogen, LH, or FSH [2] [5].
Gonadorelin Hydrochloride, Gonadorelin Acetate, and Gonadorelin Diacetate Forms
Names such as gonadorelin hydrochloride, gonadorelin acetate, and gonadorelin diacetate generally refer to salt or formulation forms of the same active GnRH peptide, although product labeling, excipients, route, and regulatory status can differ by manufacturer and country [1] [2] [3]. The clinically important question is not only the chemical salt, but whether the specific gonadorelin product is approved, labeled for human use, properly manufactured, and used in the right medical context [3] [13].
Why Does This Peptide Differ From Long-Acting GnRH Analogs?
Gonadorelin differs from long-acting GnRH analogs such as leuprolide because its short-acting, physiologic role is to reproduce GnRH signaling, while continuous stimulation with long-acting GnRH agonists can ultimately suppress gonadotropin secretion through receptor desensitization [6] 17. That distinction matters because pulsatile GnRH signaling can stimulate gonadotropin release, whereas sustained GnRH agonist exposure is used clinically in very different settings, including sex-steroid suppression [6] [17].
How Does Gonadorelin Peptide Work in the Reproductive Hormone Axis?
Gonadorelin acts within the hypothalamic-pituitary-gonadal axis, often shortened to the HPG axis [5]. This axis links the brain, pituitary gland, ovaries or testicles, and downstream hormones such as estrogen and testosterone through feedback loops [5].
How Gonadorelin Works Between the Hypothalamus and Pituitary Gland
Under normal physiology, the hypothalamus releases GnRH into the pituitary portal circulation, where it reaches gonadotroph cells in the anterior pituitary [5]. Gonadorelin works by mimicking that hypothalamic signal, allowing clinicians or researchers to observe whether the pituitary can respond by releasing luteinizing hormone and follicle-stimulating hormone [4] [5].
Why Does Pulsatile Secretion Matter More Than Continuous Administration of Gonadorelin?
Pulsatile secretion is central to GnRH biology because the frequency and pattern of GnRH exposure influence LH and FSH synthesis and release [5] [6]. Continuous administration of gonadorelin or a GnRH agonist can reduce pituitary responsiveness over time, so the same molecule class can have different effects depending on timing, dose pattern, and duration [6] [17].
Mechanism of Action: Gonadorelin, the Anterior Pituitary, and Gonadotropin Release
The mechanism of action is best understood as upstream endocrine signaling rather than direct gonadal stimulation [5]. Gonadorelin targets the pituitary GnRH receptor, and the pituitary response then affects LH and FSH, which act on the gonads [5] [6].
How Gonadorelin Binds and Activates the GnRH Receptor
Gonadorelin binds the gonadotropin-releasing hormone receptor on pituitary gonadotroph cells [2] [5]. This receptor is a G protein-coupled receptor, and its activation triggers intracellular signaling that supports gonadotropin synthesis and secretion [5] [6].
Gonadorelin Stimulates the Anterior Pituitary to Release LH and FSH
Gonadorelin stimulates the anterior pituitary to release LH and FSH when the pituitary gland is capable of responding [4] [5]. LH and FSH then act on the ovaries or testicles, helping regulate ovulation, estrogen production, testosterone production, and spermatogenesis in appropriate physiologic or clinical settings [5] [8].
What Is Gonadorelin Used For in Medicine and Research?
The use of gonadorelin depends on whether the discussion is about an approved diagnostic product, clinician-supervised pulsatile therapy, a research protocol, or an unsupported online claim [3] [4] [8]. These categories should not be blended together because each has a different evidence and safety profile.
Approved Diagnostic Contexts Where Clinicians Use Gonadorelin
FDA records for Factrel identify gonadorelin hydrochloride as a drug product with approved labeling, and U.S. labeling has described its use for evaluating the functional capacity and response of pituitary gonadotrope cells [3] [4]. In that diagnostic context, the clinical endpoint is usually a measured LH response after administration, not a fertility or testosterone “optimization” outcome [4].
How Does the Use of Gonadorelin Differ From Broader Hormone Therapies?
Gonadorelin therapy differs from hormone therapies such as testosterone, HCG, FSH, estrogen therapy, aromatase inhibitors, or long-acting GnRH analogs because it acts upstream at the pituitary GnRH receptor [5] 15 18. For example, human chorionic gonadotropin can act more like an LH signal at the gonadal level, while gonadorelin requires a responsive pituitary gland to increase LH and FSH [5] [15].
Potential Benefits of Gonadorelin Peptide
The potential benefits of gonadorelin are strongest when the claim matches a studied or labeled medical context [3] [4] [8]. Claims become much weaker when they are generalized to people without diagnosed hypothalamic or pituitary disorders, fertility evaluation, or clinician-supervised monitoring [8] [13].
Gonadorelin Benefits Most Supported by Hormone Testing Data
The clearest benefit of approved gonadorelin hydrochloride labeling is diagnostic: it can help evaluate whether the anterior pituitary releases gonadotropins after GnRH stimulation [3] [4]. In selected patients with hypogonadotropic hypogonadism, pulsatile GnRH or gonadorelin approaches have also been studied as a way to restore more physiologic LH and FSH stimulation, but this depends on intact pituitary function and careful monitoring [8] 9.
Why Should Benefits of Gonadorelin Not Be Generalized?
Benefits of gonadorelin should not be generalized because GnRH biology is diagnosis-specific and pattern-specific [5] [6]. For men on TRT or men on testosterone replacement therapy, exogenous testosterone can suppress spermatogenesis, and claims that gonadorelin reliably preserves fertility in all men undergoing testosterone replacement therapy are not established by strong clinical evidence [18] 19.
Gonadorelin for Men: Fertility, Testosterone, and Spermatogenesis
Gonadorelin for men is usually discussed in relation to hypogonadotropic hypogonadism, fertility goals, pituitary responsiveness, and sperm production in men 7 [8] [9]. It should not be interpreted as a general testosterone booster or a substitute for diagnosing the cause of low testosterone [8] [18].
What Have Human Studies Shown in Hypogonadal Men?
Human studies and expert reviews have described pulsatile GnRH therapy as one option for men with congenital or idiopathic hypogonadotropic hypogonadism when the pituitary can respond to GnRH stimulation [7] [8] [9]. The goal in that setting is to stimulate endogenous LH and FSH signaling, which may support testicular testosterone production and spermatogenesis under specialist supervision [8] [9].
Pulsatile Gonadorelin, Long-Term GnRH Therapy, and Sperm Production in Men
A two-year comparative study in men with isolated hypogonadotropic hypogonadism evaluated pulsatile GnRH therapy against exogenous gonadotropins and reported differences in testicular and spermatogenic responses over time 10. This type of finding is why some summaries state that a gonadorelin pump induces earlier spermatogenesis, but that phrase should be read as a study-context observation, not as a guaranteed outcome for all hypogonadal men [10] [8].
Gonadorelin in Female Reproductive Care and Ovulation Disorders
In female reproductive care, pulsatile gonadorelin has been studied mainly in hypothalamic causes of anovulation, such as functional hypothalamic amenorrhea and hypogonadotropic hypogonadism [11] [8]. The rationale is to replace missing GnRH pulse signaling rather than to directly stimulate the ovary like exogenous gonadotropin medications [5] [11].
How Has Pulsatile Gonadorelin Been Studied for Ovulation?
Clinical guidance on functional hypothalamic amenorrhea discusses fertility treatment options, including approaches that restore gonadotropin stimulation in carefully selected patients [11]. Pulsatile gonadorelin can be biologically appropriate when the problem is deficient hypothalamic GnRH output and the pituitary and ovaries remain responsive [5] [11].
Fertility Outcomes in Hypothalamic Amenorrhea and Hypogonadotropic Hypogonadism
Fertility outcomes in hypothalamic amenorrhea or hypogonadotropic hypogonadism depend on diagnosis, baseline hormone status, body weight or energy availability, pituitary response, ovarian response, and monitoring [8] [11]. Evidence supports specialist evaluation because ovulation induction and fertility treatment involve risks such as multifollicular response, pregnancy complications, and the need for individualized monitoring [11].
What Does Human Research Say About Gonadorelin Therapy?
Human research on gonadorelin is strongest where the drug is used as a diagnostic GnRH challenge or as pulsatile GnRH replacement in clearly defined reproductive endocrine disorders [3] [4] [8]. It is weaker when extrapolated to anti-aging, bodybuilding, routine TRT support, libido, mood, or general hormone optimization claims [13] [18] [19].
| Evidence Area | What Has Been Studied | Evidence Level | What It Can and Cannot Show |
|---|---|---|---|
| Pituitary gonadotrope testing | Gonadorelin hydrochloride labeling describes diagnostic testing of pituitary LH response after GnRH stimulation [3] [4]. | Approved medical use | Can help assess pituitary response; cannot by itself diagnose every cause of reproductive hormone dysfunction. |
| Male hypogonadotropic hypogonadism | Pulsatile GnRH therapy and gonadotropin therapy have been studied in selected men with congenital or idiopathic hypogonadotropic hypogonadism [8] [9] [10]. | Clinical / early human evidence | Can support fertility induction in selected patients; cannot be generalized to all men with low testosterone. |
| Female hypothalamic amenorrhea | Clinical guidance discusses fertility treatment strategies for functional hypothalamic amenorrhea, including GnRH-based approaches where available [11]. | Clinical evidence | Can inform specialist care; cannot replace evaluation of energy deficit, bone health, and other causes of amenorrhea. |
| HCG and gonadotropin alternatives | HCG and gonadotropins act downstream of gonadorelin and are used in some reproductive endocrine contexts [15] 16 [19]. | Approved / clinical evidence depending on product and indication | Helps compare mechanisms; does not prove one therapy is best for an individual. |
| Online TRT or “optimization” claims | Testosterone therapy can suppress spermatogenesis, but routine claims that gonadorelin prevents this in all men on testosterone are not established [18] [19]. | Unsupported or evidence-limited | Raises a clinician-discussion topic; does not establish a self-treatment protocol. |
Evidence Strength by Indication and Study Design
Evidence strength is highest when a claim is supported by approved labeling, well-described clinical populations, and objective hormone or fertility endpoints [3] [4] [8]. ClinicalTrials.gov can help identify registered studies involving gonadorelin, but registry listings should be interpreted by status, population, design, and results availability rather than treated as proof of effectiveness 12.
Did Gonadorelin Pump Studies Report Earlier Spermatogenesis?
Some literature comparing pulsatile GnRH delivery with exogenous gonadotropins in men with isolated hypogonadotropic hypogonadism reported differences in timing of sperm production and testicular response [10]. The key limitation is that these findings apply to specialized endocrine infertility populations, not to unsupervised peptide use, men without hypogonadotropic hypogonadism, or men seeking general performance benefits [8] [10].
What Does Preclinical and Mechanistic Research Add?
Preclinical and mechanistic research helps explain why gonadorelin can affect reproductive hormones, but it cannot prove clinical benefit in people by itself [5] [6]. Mechanism matters most when it is paired with the correct diagnosis, route, dose pattern, and clinical endpoint [4] [8].
Animal and Cell Signaling Models for Gonadotropin Release
Animal, cell, and receptor studies have helped define how GnRH receptor activation in pituitary gonadotrophs leads to gonadotropin release [5] [6]. These models support biological plausibility for gonadorelin targets, but translation to human fertility or testosterone outcomes depends on clinical trial and patient-level data [6] [8].
Why Does Mechanism Not Always Predict Clinical Outcomes?
A molecule can have a plausible mechanism and still fail to produce a desired outcome in a given person or indication [6]. With gonadorelin, the pituitary must respond, the pattern must be physiologic when stimulation is intended, and downstream gonadal tissue must be capable of responding to LH and FSH [5] [8].
Side Effects of Gonadorelin and Reported Adverse Reactions
Side effects of gonadorelin should be interpreted from product labeling, supervised clinical use, and the route of administration [4]. The risk profile may differ between a single diagnostic gonadorelin injection, pulsatile infusion protocols, compounded gonadorelin, and unapproved products [4] [13].
Common Side Effects Reported With Gonadorelin Injection
Labeling for gonadorelin hydrochloride has described generally transient adverse reactions such as headache, flushing, nausea, abdominal discomfort, dizziness, or local injection reactions, although product-specific labeling should be checked for the exact wording and frequency [4]. Hypersensitivity reactions are medically important for any injectable medication and should be evaluated by a clinician [4].
Which Hormone-Related, Mood, or Injection-Site Effects Matter?
Because gonadorelin acts through the reproductive hormone axis, hormone-related symptoms should be interpreted in context of LH, FSH, testosterone, estrogen, menstrual function, testicular function, or ovarian response [5] [8]. Injection-site effects depend on route and formulation, and study administration methods should not be converted into self-administration instructions [4] [13].
Safety Risks, Contraindications, and Medical Supervision
Medical supervision matters because gonadorelin can affect the endocrine system and because the interpretation of hormone responses requires appropriate testing [4] [5]. Safety also depends on whether the product is approved, compounded, investigational, or unapproved [3] [13].
Who Should Discuss Contraindications Before Gonadorelin?
People with prior hypersensitivity to gonadorelin or formulation components should discuss this with a clinician because hypersensitivity is a standard contraindication or warning area in medication labeling [4]. A clinician should also review pituitary disease, unexplained reproductive symptoms, infertility history, current hormone therapies, and current medications before interpreting any use of gonadorelin [4] [5] [8].
Hormone-Sensitive Cancer, Pregnancy, Breastfeeding, and Pediatric Considerations
People with hormone-sensitive cancer history, breast cancer, prostate cancer, pituitary neoplasm, pregnancy, breastfeeding, or pediatric endocrine concerns should not interpret gonadorelin information without specialist input [4] [17]. The reason is not that every one of these conditions has the same contraindication, but that changing or testing reproductive hormone signaling can affect medical decisions and requires individualized risk assessment [5] [11].
Drug Interactions and Gonadorelin vs Hormone Therapy Combinations
Drug interactions with gonadorelin are best understood as endocrine-context interactions: other medicines or hormones may alter baseline LH, FSH, testosterone, estrogen, or pituitary responsiveness [4] [5]. This is especially relevant for people using testosterone, estrogen, HCG, gonadotropins, aromatase inhibitors, or other hormone therapies [18] [19].
Gonadorelin vs HCG: Human Chorionic Gonadotropin Strategies
Gonadorelin vs HCG is an upstream-versus-downstream comparison [5] [15]. Gonadorelin binds the GnRH receptor at the pituitary to stimulate LH and FSH release if the pituitary can respond, while human chorionic gonadotropin acts more like LH at the gonadal level and has its own labeled uses, risks, and dosing context [5] [15] [16].
Androgens, Estrogen, Aromatase Inhibitors, and Gonadotropin Medications
Androgens, estrogen therapies, aromatase inhibitors, HCG, and gonadotropin medications can all influence reproductive hormone interpretation or fertility treatment decisions [18] [19]. In men on testosterone therapy, major endocrine and urology guidelines recognize that exogenous testosterone can suppress spermatogenesis, so fertility-preservation questions should be handled through clinician-guided evaluation rather than online peptide protocols [18] [19].
What Gonadorelin Dosage Information Appears in Labels and Published Studies?
Gonadorelin dosage information should be separated into approved-label diagnostic dosing and published-study or specialist-treatment protocols [4] [8] [11]. Study doses should not be interpreted as personal dosing advice.
Approved Label Dosage for Gonadorelin Hydrochloride
U.S. gonadorelin hydrochloride labeling for Factrel has described a single 100 microgram intravenous dose for adult diagnostic evaluation of pituitary gonadotrope response, with blood sampling used to measure hormone response in a clinical setting [4]. That label context is diagnostic and clinician-managed; it is not a general fertility, TRT, or wellness dosing protocol [3] [4].
Why Is Gonadorelin Dosage Information Not Personal Medical Advice?
Dosage decisions for gonadorelin depend on indication, product, route, monitoring plan, baseline hormones, age, sex, fertility goals, pituitary function, gonadal function, and regulatory status [4] [8] [11]. Published study protocols and approved labels are useful for understanding the literature, but they do not determine what any individual should use [4] [13].
Administration of Gonadorelin in Medical Literature
Administration of gonadorelin in the literature includes diagnostic injection contexts and pulsatile pump or infusion contexts in specialist reproductive endocrinology research and care [4] [8] [11]. Route matters because a single diagnostic injection is not the same as pulsatile gonadorelin therapy designed to mimic physiologic GnRH pulses [4] [6].
Gonadorelin Injection, Subcutaneous Gonadorelin, and Infusion Contexts
Gonadorelin injection in approved diagnostic labeling has been described as intravenous administration for pituitary response testing [4]. Published reproductive-endocrine literature also discusses pulsatile gonadorelin delivered by pump, including subcutaneous gonadorelin or infusion approaches in selected settings, but those are clinician-managed medical protocols rather than self-use instructions [8] [9] [11].
Why Is This Not a Self-Administration or Reconstitution Guide?
This article does not provide reconstitution, mixing, injection, cycling, stacking, or self-administration instructions because those details can create unsafe personal medical guidance [13]. Administration route, product quality, sterility, monitoring, and adverse-event response all require licensed clinical oversight, especially when compounded or unapproved products are involved [4] [13].
Is Gonadorelin FDA-Approved or Legally Available?
Regulatory status is product-specific and indication-specific [3]. A blanket statement such as “gonadorelin is not FDA-approved” is less accurate than saying that FDA has records for an approved gonadorelin hydrochloride product, while compounded gonadorelin is not FDA-approved as a compounded drug [3] [13].
Approved Gonadorelin for Human Use, Discontinued Labels, and Country Differences
FDA’s Drugs@FDA database provides application-level information for Factrel, a gonadorelin hydrochloride product, and should be checked for label documents and marketing status [3]. Country differences also matter because a formulation, brand, route, or indication that appears in one jurisdiction may not be approved, marketed, or available in another [3] [4].
Compounded Gonadorelin and Unapproved Product Quality Risks
Compounded gonadorelin products are not FDA-approved, and FDA states that compounded drugs are not reviewed for safety, effectiveness, or manufacturing quality before marketing in the same way approved drugs are [13]. FDA also maintains information on bulk drug substances used in compounding, which is relevant because compounding legality and quality expectations depend on the specific legal pathway and substance status 14.
Evidence Limitations and Practical Clinician Discussion Points
The safest way to interpret gonadorelin research is to separate approved diagnostic use, clinician-supervised fertility therapy, mechanistic research, and unsupported online claims [3] [4] [8] [13]. The strongest conclusions come from labeling and well-described human endocrine studies, while weaker claims need cautious language and clinician review [4] [8] [11].
Where Is Gonadorelin Research Stronger, Limited, or Unsupported?
Research on gonadorelin is stronger for pituitary response testing and selected hypogonadotropic reproductive disorders than for broad testosterone optimization, anti-aging, libido, bodybuilding, or routine support for men on TRT [3] [4] [8] [18]. Long-term safety data are also harder to generalize when products, routes, dosing patterns, and patient populations differ [4] [8] [13].
What Questions Should Readers Ask About Testing, Monitoring, Fertility Goals, and Alternatives?
Readers discussing gonadorelin with a licensed clinician can use this checklist:
- What diagnosis or hormone pattern is being evaluated?
- Is the goal pituitary testing, fertility treatment, ovulation induction, spermatogenesis, or another endpoint?
- Is the product approved, investigational, compounded, or unapproved?
- What baseline labs are needed, such as LH, FSH, testosterone, estrogen, prolactin, or pituitary evaluation?
- Could current hormone therapies, including testosterone, estrogen, HCG, aromatase inhibitors, or gonadotropins, affect interpretation?
- What side effects or warning signs require medical follow-up?
- Are approved alternatives or guideline-supported fertility treatments more appropriate?
Gonadorelin helps illustrate why peptide information should be read through evidence quality, regulatory status, safety data, and clinician-guided decision-making rather than through online dosing claims or product marketing [4] [8] [13] [19].
REFERENCES
- National Center for Biotechnology Information. PubChem Compound Summary: Gonadorelin. PubChem. Accessed 2026.
- DrugBank. Gonadorelin: DrugBank Drug Entry DB00644. DrugBank Online. Accessed 2026.
- U.S. Food and Drug Administration. Drugs@FDA: Factrel, NDA 017925. FDA Drugs@FDA. Accessed 2026.
- National Library of Medicine. DailyMed records for Factrel / gonadorelin hydrochloride prescribing information. DailyMed. Accessed 2026.
- StatPearls Publishing. Physiology, Gonadotropin-Releasing Hormone. NCBI Bookshelf. Updated regularly.
- Conn PM, Crowley WF Jr. Gonadotropin-releasing hormone and its analogs. New England Journal of Medicine. 1991;324(2):93-103. doi:10.1056/NEJM199101103240205.
- Seminara SB, Hayes FJ, Crowley WF Jr. Gonadotropin-releasing hormone deficiency in the human: pathophysiological and genetic considerations. Endocrine Reviews. 1998;19(5):521-539. doi:10.1210/edrv.19.5.0344.
- Boehm U, Bouloux PM, Dattani MT, et al. Expert consensus document: European Consensus Statement on congenital hypogonadotropic hypogonadism—pathogenesis, diagnosis and treatment. Nature Reviews Endocrinology. 2015;11:547-564. doi:10.1038/nrendo.2015.112.
- Fraietta R, Zylberstejn DS, Esteves SC. Hypogonadotropic hypogonadism revisited. Clinics. 2013;68(Suppl 1):81-88. PMCID: PMC3583156.
- Liu L, Banks SM, Barnes KM, Sherins RJ. Two-year comparison of testicular responses to pulsatile gonadotropin-releasing hormone and exogenous gonadotropins in men with isolated hypogonadotropic hypogonadism. Journal of Clinical Endocrinology & Metabolism. 1988;67(6):1140-1145. PMID:3141451.
- Gordon CM, Ackerman KE, Berga SL, et al. Functional Hypothalamic Amenorrhea: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism. 2017;102(5):1413-1439. doi:10.1210/jc.2017-00131.
- U.S. National Library of Medicine. ClinicalTrials.gov search results for gonadorelin. ClinicalTrials.gov. Accessed 2026.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers. FDA. Accessed 2026.
- U.S. Food and Drug Administration. Bulk Drug Substances Used in Compounding Under Section 503A of the FD&C Act. FDA. Accessed 2026.
- StatPearls Publishing. Human Chorionic Gonadotropin. NCBI Bookshelf. Updated regularly.
- National Library of Medicine. DailyMed records for Pregnyl / chorionic gonadotropin prescribing information. DailyMed. Accessed 2026.
- StatPearls Publishing. Leuprolide. NCBI Bookshelf. Updated regularly.
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism. 2018;103(5):1715-1744. doi:10.1210/jc.2018-00229.
- American Urological Association and American Society for Reproductive Medicine. Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline. AUA/ASRM Guideline. Updated 2020; amended 2024.
FAQs
What does Gonadorelin peptide do?
Gonadorelin peptide mimics GnRH, the hypothalamic hormone signal that prompts the anterior pituitary to release LH and FSH when the pituitary can respond [1] [5]. In practical terms, gonadorelin activates the GnRH receptor upstream of the ovaries or testicles rather than acting like testosterone, estrogen, or HCG itself [5]. Its clinical meaning depends on whether it is used for diagnostic testing, fertility-related care, or research.
Can gonadorelin increase testosterone or restore fertility?
Gonadorelin may increase testosterone in selected people whose pituitary and gonads can respond, especially certain hypogonadotropic hypogonadism contexts studied under specialist care [8] [9]. It is not established as a general testosterone-support option for men on testosterone therapy. Claims that gonadorelin restores fertility during TRT are evidence-limited because exogenous testosterone can suppress spermatogenesis, and fertility-preservation decisions should follow guideline-informed clinician evaluation [18] [19].
How does gonadorelin compare with HCG?
Gonadorelin is not universally better or worse than HCG; they work at different points in the reproductive hormone axis. Gonadorelin signals the pituitary GnRH receptor to release LH and FSH if the pituitary is responsive, while human chorionic gonadotropin acts more like LH at the gonadal level [5] [15]. Whether either therapy is appropriate depends on diagnosis, fertility goals, product labeling, monitoring, and clinician judgment [16] [19].
What potential side effects or adverse events can occur with gonadorelin?
Potential side effects of gonadorelin can include transient symptoms such as headache, flushing, nausea, dizziness, abdominal discomfort, or injection site reactions, based on product-label safety information [4]. Serious side effects are uncommon in routine label discussions but require prompt medical evaluation if they occur. Adverse events may be harder to interpret with compounded or unapproved products because quality, sterility, labeling, and monitoring can differ from approved-drug standards [13].
What dosage or administration route information is available for gonadorelin?
Dosage and administration route information should come from approved labeling or published studies, not personal-use protocols. U.S. gonadorelin hydrochloride labeling has described a single 100 microgram intravenous diagnostic dose with hormone-response blood sampling [4]. Published literature also discusses infusion of gonadorelin or pump-based pulsatile delivery in selected reproductive endocrine settings [8] [11]. Questions about half-life, frequency, or route should be interpreted through clinician-supervised medical context.
Is gonadorelin FDA-approved, legal, or available by prescription?
Gonadorelin’s FDA approval and legal status are product-specific. FDA records exist for a gonadorelin hydrochloride product used in diagnostic pituitary testing, but compounded gonadorelin products are not FDA-approved as compounded drugs [3] [13]. A clinician may discuss clinical use or off-label use only within applicable law, evidence, product availability, and patient-specific risk assessment. Regulatory status should not be interpreted as a reason to obtain unapproved products without medical oversight [14].
Contributing Authors
The following authors are recognized for published research that helped shape the scientific and clinical context discussed in this article.
William F. Crowley Jr.
Author profile: PubMed Author Search
William F. Crowley Jr. is a research author whose published work is closely connected to GnRH physiology, gonadotropin signaling, and the clinical evidence base surrounding hypogonadotropic reproductive disorders. His publications are relevant to understanding why Gonadorelin peptide is interpreted differently from long-acting GnRH analogs and why pulsatile GnRH signaling is central to pituitary LH and FSH release. His work also provides useful context for evidence limitations in GnRH-deficiency conditions, where clinical interpretation depends on diagnosis, pituitary responsiveness, treatment setting, and monitored endocrine endpoints.
Selected publications:
- Gonadotropin-releasing hormone and its analogs — New England Journal of Medicine, 1991. DOI: 10.1056/NEJM199101103240205.
- Gonadotropin-releasing hormone deficiency in the human: pathophysiological and genetic considerations — Endocrine Reviews, 1998. DOI: 10.1210/edrv.19.5.0344.
Nelly Pitteloud
Author profile: PubMed Author Search
Nelly Pitteloud is a clinical research author whose publications are relevant to congenital and idiopathic hypogonadotropic hypogonadism, GnRH deficiency, and reproductive endocrine evaluation. Her work helps frame how clinical evidence should be interpreted in selected patient populations rather than generalized to broad hormone-optimization claims. The publications highlighted here are useful for understanding the diagnostic and therapeutic context around GnRH-pathway disorders, including evidence quality, reversibility, fertility-related endpoints, and the need for clinician-guided interpretation of reproductive hormone findings.
Selected publications:
- European Consensus Statement on congenital hypogonadotropic hypogonadism—pathogenesis, diagnosis and treatment — Nature Reviews Endocrinology, 2015. DOI: 10.1038/nrendo.2015.112.
- Reversal of idiopathic hypogonadotropic hypogonadism — New England Journal of Medicine, 2007. DOI: 10.1056/NEJMoa066494.