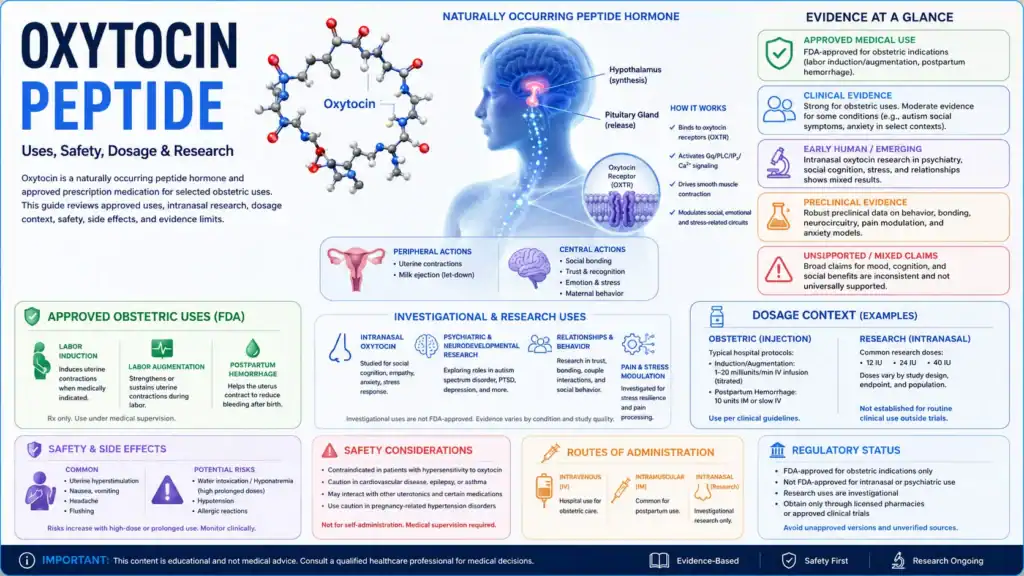
Oxytocin peptide is a naturally occurring peptide hormone and neuropeptide that also exists as a prescription medication for specific obstetric uses. This educational article explains oxytocin biology, approved medical uses, intranasal oxytocin research, dosage information from labels or studies, safety concerns, contraindications, and evidence limits without giving personalized medical advice.
- Oxytocin is a cyclic nonapeptide hormone listed in PubChem as C43H66N12O12S2 and is produced naturally in the hypothalamus 1.
- Prescription oxytocin injection is approved for selected medical obstetric uses, including medically indicated labor induction or augmentation, management of incomplete or inevitable abortion, and postpartum uterine bleeding or hemorrhage 2.
- Oxytocin acts through the oxytocin receptor, a G protein-coupled receptor involved in uterine contraction, lactation, and central nervous system signaling 3.
- Intranasal oxytocin has been studied for social cognition, autism spectrum disorder, schizophrenia, trust, and social behavior, but results are mixed and do not establish broad treatment use 4.
- The strongest evidence for oxytocin as a medication comes from approved obstetric labeling and guideline-based uterotonic use, not from online claims about bonding, empathy, or social enhancement [2].
- Side effects and risks depend strongly on route and setting; parenteral oxytocin can cause uterine hyperstimulation, water intoxication, arrhythmias, and fetal or neonatal adverse events when misused or poorly monitored 5.
- Dosage information should be interpreted as approved-label or study context only, not as a personal protocol.
Fast Answer
Oxytocin peptide is a naturally produced peptide hormone and neuropeptide that is also available as a prescription oxytocin medication for specific obstetric indications. It is commonly searched because of its roles in labor, lactation, social behavior, trust, autism spectrum disorder research, and intranasal oxytocin studies. Evidence is strongest for approved obstetric use, while behavioral and psychiatric uses remain investigational or mixed. Safety depends on route, dose, monitoring, pregnancy status, and clinical context [1], [2], [4].
Evidence basis note: This page uses approved drug labeling, regulatory drug-label sources, scientific databases, clinical-trial records, and peer-reviewed literature. Claims without reliable clinical support are described as preliminary, mixed, or unsupported rather than established.
What Is the Oxytocin Peptide?
Oxytocin peptide is a short cyclic peptide hormone that functions both as a peripheral hormone and a central neuromodulator. PubChem identifies oxytocin as a heterodetic cyclic peptide and peptide hormone, and clinical references describe its synthesis in the hypothalamus and release through the posterior pituitary [1], [3].
Oxytocin as a Peptide Hormone and Neuropeptide
Oxytocin is a nine-amino-acid peptide hormone that belongs to the neurohypophyseal hormone family. It is closely related to vasopressin, another posterior-pituitary peptide hormone, but oxytocin’s best-established physiologic roles involve uterine contraction and milk ejection rather than water retention [3], 6.
As a neuropeptide, oxytocin is also studied in brain circuits involved in social behavior, emotional salience, stress responses, reward processing, and human bonding. That research is biologically plausible, but it is not the same as having an approved treatment claim for autism, schizophrenia, trust, or relationship outcomes [4].
Endogenous Oxytocin vs Oxytocin Medication
Endogenous oxytocin is produced by the body, while oxytocin medication refers to synthetic oxytocin used under medical supervision. DailyMed labeling describes oxytocin injection as a synthetic sterile solution intended for intravenous infusion or intramuscular use, with each mL containing activity equivalent to 10 USP oxytocin units [2].
This distinction matters. Normal oxytocin release during childbirth, lactation, touch, or social contexts is not equivalent to administering oxytocin as a drug, and intranasal oxytocin research does not automatically translate into routine clinical use [4], [6].
Why Oxytocin Is Discussed in Therapeutic Research
Oxytocin is discussed therapeutically because it has approved medical roles and because the oxytocin system is involved in human social cognition and behavior. Reviews of intranasal oxytocin research note that interest grew from studies suggesting effects on social cognition, emotion recognition, attention to social cues, and psychiatric conditions marked by social dysfunction [4].
The evidence does not support a simple “love hormone” interpretation. Oxytocin may increase attention to socially relevant information, but effects can vary by person, context, sex, diagnosis, dose, route, and study design [4].
Oxytocin Biology and Endogenous Release
Oxytocin biology begins in the hypothalamus and extends to the posterior pituitary, uterus, breast, reproductive tissues, and brain circuits involved in behavior. The posterior pituitary stores and releases oxytocin synthesized in hypothalamic neurons [3].
Hypothalamus, Posterior Pituitary, and Oxytocin Neurons
Oxytocin is produced mainly in hypothalamic nuclei and transported along axons to the posterior pituitary for release into circulation. NCBI Bookshelf describes oxytocin as being synthesized in the paraventricular nuclei and stored for release from the pituitary gland [3].
In addition to peripheral release, oxytocin neurons can influence central nervous system signaling through axonal and dendritic release mechanisms. This central-peripheral split helps explain why plasma oxytocin levels may not perfectly represent oxytocin signaling in the brain [4].
Paraventricular and Supraoptic Nucleus Signaling
The paraventricular nucleus and supraoptic nucleus are key hypothalamic regions in the oxytocin system. Posterior pituitary physiology sources describe hypothalamic synthesis, axonal transport, storage, and release of posterior-pituitary hormones, including oxytocin [3].
In behavioral research, the same oxytocin system is studied in connection with the amygdala, ventral tegmental area, nucleus accumbens, stria terminalis, and other regions involved in social salience, reward, and threat processing. The challenge is that identifying a neural pathway does not prove that a medication improves a clinical outcome [4].
Oxytocin Levels, Plasma Measures, and Interpretation Limits
Oxytocin levels can be measured in plasma, cerebrospinal fluid, or other biological samples, but interpretation is difficult. Reviews of intranasal oxytocin research note methodological concerns about whether peripheral oxytocin concentrations reliably estimate central oxytocin levels [4].
This is why plasma oxytocin levels, oxytocin concentration, or changes in oxytocin should not be treated as simple diagnostic markers. They may support research questions, but they do not by themselves establish who needs oxytocin treatment or who will respond.
How Does Oxytocin Peptide Work?
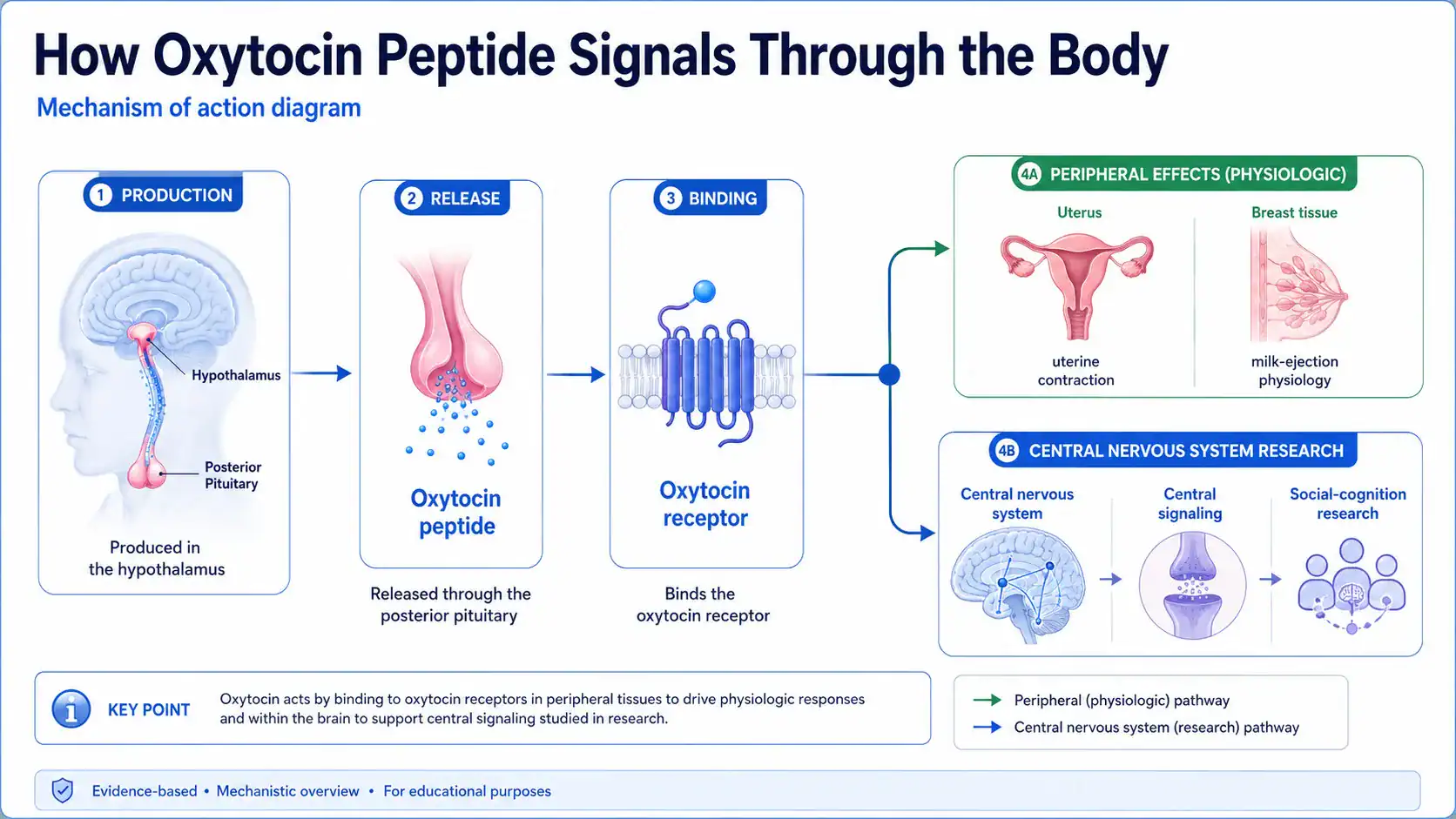
Oxytocin peptide works by binding the oxytocin receptor, which triggers cell-signaling pathways in target tissues and neural circuits. In uterine smooth muscle, oxytocin receptor signaling increases intracellular calcium and promotes contraction [3], 7.
Oxytocin Receptor Activity and Cell Signaling
The oxytocin receptor is a G protein-coupled receptor that primarily couples to Gq/11-family signaling, leading to intracellular pathways involved in calcium mobilization [7]. In the uterus, oxytocin binding activates phospholipase C signaling, inositol triphosphate activity, and calcium release, which supports smooth muscle contraction [3].
Oxytocin receptor expression changes across tissues and physiological states. In late pregnancy, uterine sensitivity to oxytocin increases, which is one reason labeled medical use requires careful dosing, monitoring, and clinical judgment [5].
Central Nervous System and Peripheral Oxytocin Effects
Oxytocin has peripheral effects in the uterus and breast, but oxytocin also modulates central nervous system circuits. Intranasal oxytocin studies often focus on social cognition because the route is intended to influence central oxytocin signaling more directly than peripheral injection [4].
In humans, early experiments reported that intranasal oxytocin affected trust behavior, and neuroimaging studies reported changes in amygdala responses to emotional faces 8, 9. These findings are important research signals, but they do not make oxytocin a general-purpose social enhancement treatment.
Why Mechanism Does Not Always Predict Clinical Benefit
A plausible mechanism does not prove clinical benefit. Oxytocin can modulate receptor signaling, amygdala activity, and social-cognitive processing in some studies, but larger trials in autism spectrum disorder and meta-analyses in schizophrenia have not shown consistent therapeutic benefit 10, 11.
The practical takeaway is evidence grading. Uterine contraction is an approved-label pharmacologic effect; social cognition is an active research area with heterogeneous results [2], [4].
Approved Medical Uses of Oxytocin
Oxytocin is an approved prescription medication for specific obstetric uses, especially when controlled uterine contraction is medically indicated. DailyMed labeling lists antepartum and postpartum indications, and these uses differ sharply from investigational intranasal oxytocin research [2].
Labor Induction, Labor Augmentation, and Uterine Contraction
Oxytocin injection is indicated for initiation or improvement of uterine contractions when medically suitable to achieve early vaginal delivery for fetal or maternal reasons [2]. The label includes medical induction, stimulation or reinforcement of labor in selected cases, and adjunctive therapy in incomplete or inevitable abortion [2].
For induction or stimulation of labor, labeling states that intravenous infusion is the acceptable parenteral route and that infusion rate and fetal heart rate require careful monitoring [5].
Postpartum Uterine Atony and Bleeding Context
Oxytocin injection is also indicated to produce uterine contractions during the third stage of labor and to control postpartum bleeding or hemorrhage [2]. WHO-linked recommendations identify oxytocin 10 IU intramuscularly or intravenously as the recommended uterotonic agent of choice for prevention of postpartum hemorrhage when multiple uterotonic options are available 12.
This is one of the clearest benefit areas for oxytocin because it is based on established obstetric pharmacology, clinical use, and guideline context rather than speculative behavioral claims.
Approved Uses vs Investigational or Off-Label Research Uses
Approved oxytocin medication is not the same as intranasal oxytocin treatment for psychiatric or behavioral indications. Reviews describe intranasal oxytocin as a research tool and possible investigational approach, while also emphasizing unresolved questions about delivery, dose, reproducibility, and patient selection [4].
For readers, the key distinction is regulatory. A drug can be approved for one indication and still be investigational, off-label, or unsupported for another.
Oxytocin Nasal Spray and Intranasal Oxytocin Research
Intranasal oxytocin research studies whether oxytocin delivered through the nose can affect central oxytocin signaling and behavior. This route has been widely used in human social cognition studies, but therapeutic translation remains uncertain [4].
How Intranasal Oxytocin Is Studied in Humans
Human intranasal oxytocin studies usually use randomized, placebo-controlled designs to test outcomes such as emotion recognition, social responsiveness, trust, neural activation, or psychiatric symptoms. ClinicalTrials.gov describes the SOARS-B autism study as testing supplemental intranasal oxytocin for social difficulties in autism spectrum disorder, with dose escalation toward 24 IU twice daily 13.
Route matters because intravenous oxytocin, intranasal oxytocin, and endogenous oxytocin release do not necessarily produce the same central or peripheral effects. A route-comparison study reported route-dependent oxytocin effects on brain and behavioral measures 14.
Oxytocin Nasal Spray on Social Behavior and Social Interaction
Oxytocin nasal spray has been studied for social behavior, social interaction, trust, empathy, and autism-related social difficulty. The early Nature trust study helped drive public interest, but later reviews caution that oxytocin’s social effects are context-dependent and not uniformly prosocial [4], [8].
In autism spectrum disorder, results have varied across age groups, protocols, and outcome measures. A large 24-week pediatric trial found no significant between-group differences in social or cognitive functioning measures between intranasal oxytocin and placebo [10].
Long-Term Intranasal Oxytocin and Chronic Oxytocin Questions
Long-term intranasal oxytocin remains an open research question. The intranasal field has moved from small proof-of-concept studies toward larger trials and more careful attention to reproducibility, dose, sex differences, and long-term safety [4].
Current evidence does not justify presenting chronic oxytocin as an established long-term therapy for autism, schizophrenia, social anxiety, trust, bonding, or relationship outcomes. Larger and more targeted studies are still needed [4], [10], [11].
Potential Benefits of Oxytocin Peptide
Potential benefits of oxytocin peptide depend on the evidence category. Approved benefits are strongest for medically supervised obstetric use, while behavioral and psychiatric benefits remain mixed, preliminary, or investigational [2], [4].
Benefits Supported by Approved Medical Use
The best-supported therapeutic benefit of oxytocin is controlled uterine contraction in selected obstetric settings. Labeling supports use for medically indicated induction or augmentation of labor, selected abortion-management contexts, and postpartum bleeding or hemorrhage control [2].
Guideline context also supports oxytocin’s role as a uterotonic for postpartum hemorrhage prevention when quality-assured oxytocin is available [12].
Social Behavior, Trust, Empathy, and Human Bonding
Oxytocin is involved in social behavior and human bonding, but the benefit claim is not simple. Intranasal oxytocin increased trusting behavior in a 2005 human trust-game experiment, while later research showed that oxytocin effects may depend on context, baseline traits, social cues, and study design [8], [4].
The most responsible interpretation is that oxytocin modulates social salience and social-cognitive processing in some settings. It should not be described as a guaranteed trust, empathy, bonding, or relationship treatment.
Lactation, Reproduction, and Sexual Behavior Research Context
Oxytocin is central to milk ejection and uterine contraction. NCBI breastfeeding physiology explains that oxytocin makes myoepithelial cells around alveoli contract, moving milk through ducts during the letdown reflex 15.
Oxytocin is also discussed in reproductive and sexual-behavior research, including roles in ejaculation and social bonding, but therapeutic claims for libido, sexual enhancement, or relationship outcomes require much stronger clinical evidence than mechanistic physiology alone [3], [4].
What Does Human Research Show About Oxytocin?
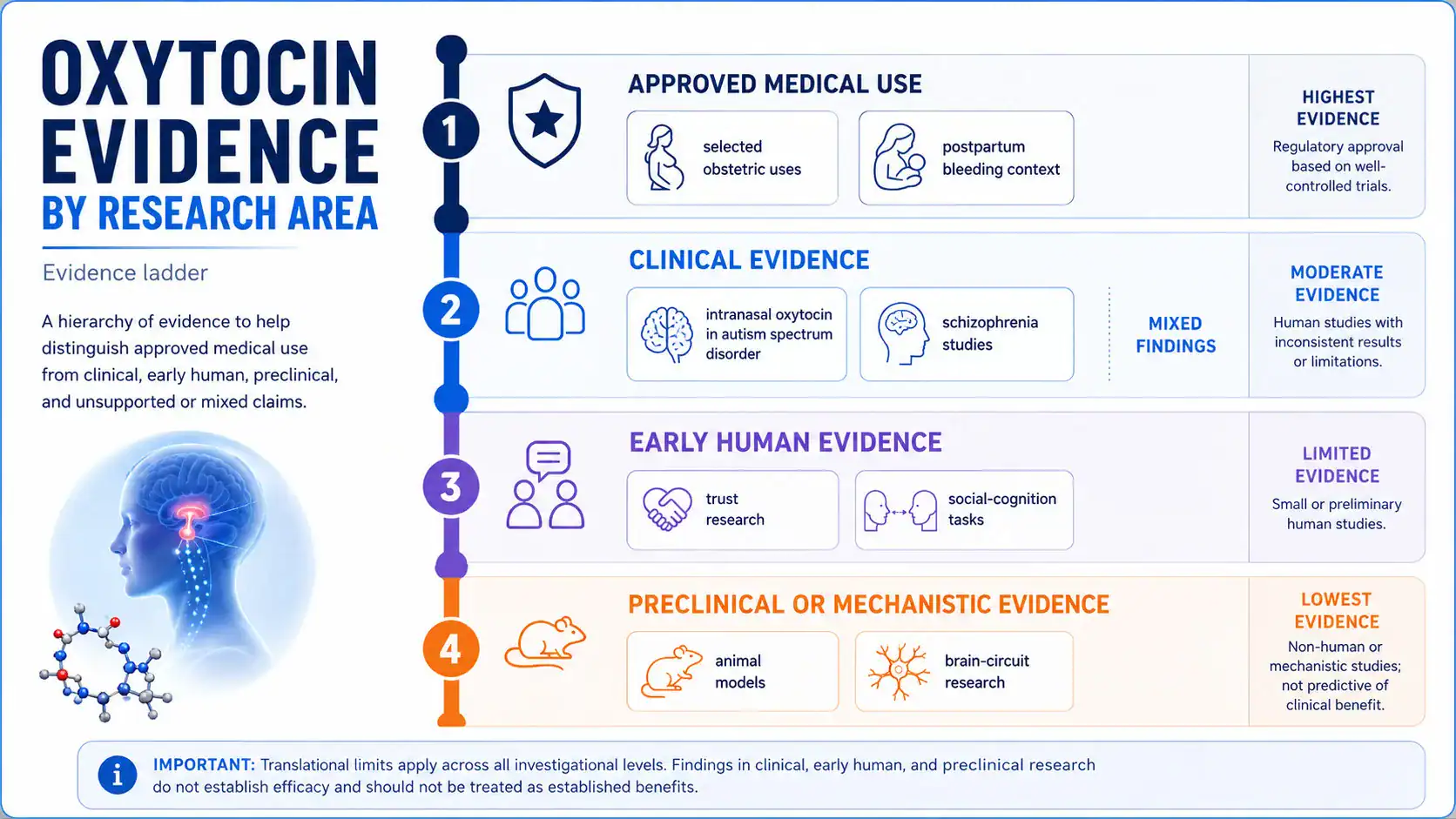
Human research shows strong evidence for approved obstetric use and mixed evidence for intranasal behavioral or psychiatric uses. Clinical meaning depends on route, population, dose, outcome measure, and whether the endpoint is physiologic, behavioral, or patient-centered [2], [4].
| Evidence Area | What Has Been Studied | Evidence Level | What It Can and Cannot Show |
|---|---|---|---|
| Obstetric use | Labor induction, augmentation, and postpartum bleeding control [2] | Approved medical use | Supports supervised medical use for labeled indications; does not support casual or unsupervised use |
| Postpartum hemorrhage prevention | Oxytocin 10 IU IM/IV as uterotonic option [12] | Guideline-supported clinical use | Supports obstetric prevention context; dose and timing depend on clinical protocols |
| Autism spectrum disorder | Pediatric and adult intranasal oxytocin trials [10], 16 | Mixed clinical evidence | Does not establish broad ASD treatment benefit |
| Schizophrenia | Meta-analysis of intranasal oxytocin for symptoms [11] | Mixed or negative clinical evidence | No consistent benefit for negative or positive symptoms |
| Trust and social cognition | Trust-game and neuroimaging studies [8], [9] | Early human / experimental | Shows possible modulation of social processing; not a treatment claim |
| Intranasal delivery | Nose-to-brain delivery and route comparisons [4], [14] | Mechanistic and translational evidence | Supports biological plausibility; does not settle therapeutic efficacy |
Clinical Trials, Study Populations, and Outcome Measures
Oxytocin clinical trials differ widely. The Sikich pediatric ASD trial studied children and adolescents ages 3 to 17 for 24 weeks with a target daily dose of 48 IU and found no significant between-group difference on social or cognitive functioning measures [10].
Adult ASD research has also used intranasal oxytocin protocols. One randomized multicenter trial enrolled 106 adults with autism spectrum disorder and assigned participants to 48 IU/day intranasal oxytocin or placebo for 6 weeks [16]. Results across the ASD literature remain heterogeneous rather than conclusively positive.
How Dose, Route, and Timing Change Study Findings
Dose, route, and timing can change oxytocin findings because central and peripheral oxytocin effects are not interchangeable. The intranasal literature includes common doses such as 24 IU in experimental work and daily totals such as 48 IU in ASD trials, but those are study protocols, not personal dosing recommendations [4], [10], [13].
Dose-response may also be non-linear. A study of an enhanced-bioavailability intranasal oxytocin spray reported an exploratory inverted U-shaped dose-response pattern, suggesting that higher doses are not automatically better 17.
Claim Strength: Established, Preliminary, Mixed, or Unsupported
Oxytocin claims should be sorted by evidence strength. Approved obstetric uses are established within labeled medical settings; intranasal oxytocin for ASD or schizophrenia is mixed; generalized claims about trust, bonding, libido, anti-aging, or “social optimization” are not established as clinical outcomes [2], [4], [10], [11].
This framework helps avoid overreading laboratory findings. Oxytocin may modulate a measurable neural or behavioral task without producing a clinically meaningful benefit in daily life.
Oxytocin in Autism Spectrum Disorder and Social Behavior Research
Oxytocin in autism spectrum disorder research has produced mixed findings, with larger and more rigorous studies tempering early optimism. The current evidence does not support presenting intranasal oxytocin as an established ASD treatment [10].
Intranasal Oxytocin in Autism Spectrum Disorder Studies
Intranasal oxytocin has been tested in ASD because oxytocin signaling, social cognition, and the oxytocin receptor gene have been studied in relation to autism. A meta-analysis reported an association between OXTR variation and autism spectrum disorder, but genetic association does not prove that oxytocin treatment improves symptoms 18.
Clinical results vary. A 2023 double-blind randomized trial in school-aged children used 12 IU twice daily for 4 weeks and found improvements in both oxytocin and placebo groups, but improvements were not specific to intranasal oxytocin during the double-blind phase 19.
Oxytocin in Children, Adults, Male, and Female Participants
Oxytocin in children, adults, male participants, and female participants may not have identical effects. Reviews of intranasal oxytocin research identify sex differences, baseline traits, psychiatric diagnosis, outcome selection, and reproducibility as major issues for future trials [4].
This is especially relevant in pediatric research. A 2021 NEJM trial in children and adolescents with ASD did not show meaningful social or cognitive benefit despite a 24-week treatment period, and adverse events were generally similar between groups [10].
Why Social Outcomes Are Difficult to Measure Reliably
Social outcomes are difficult to measure because “social functioning” includes attention, emotion recognition, eye gaze, motivation, communication, repetitive behavior, caregiver ratings, and real-world interaction. A change on one laboratory task may not translate into daily-life improvement [4].
Oxytocin also does not simply increase positive social behavior. Reviews note that oxytocin can sharpen social salience and may have different effects depending on social context, including in-group/out-group conditions and emotional threat cues [4].
Preclinical Evidence and Translational Limits
Preclinical evidence supports oxytocin’s biological importance in mammalian social behavior, reproduction, and neural signaling, but animal findings cannot be treated as proof of human therapeutic benefit. Translational limits are especially important for behavioral claims [4].
Animal Models, Oxytocin Receptor-Deficient Mice, and Behavior
Animal models have helped identify oxytocin receptor pathways, social-recognition effects, reproductive physiology, and neural-circuit roles. Oxytocin receptor-deficient mice and other experimental models are useful for mechanism discovery, but they cannot answer whether intranasal oxytocin improves complex human social outcomes [4], [18].
Animal evidence is strongest when used to explain plausible mechanisms. It becomes weaker when used to make direct claims about clinical treatment, dosing, or long-term outcomes in people.
Amygdala, Ventral Tegmental Area, and Reward Circuit Findings
Oxytocin research frequently examines the amygdala, ventral tegmental area, nucleus accumbens, and related reward or salience circuits. In a human fMRI study, intranasal oxytocin reduced right-sided amygdala responses to emotional faces, supporting a role in social-emotional processing [9].
These brain findings help explain why oxytocin is studied for social cognition. They do not show that oxytocin nasal spray reliably improves autism, schizophrenia, empathy, trust, or relationship functioning in clinical practice.
Oxytocin Dosage Information From Labels and Published Studies
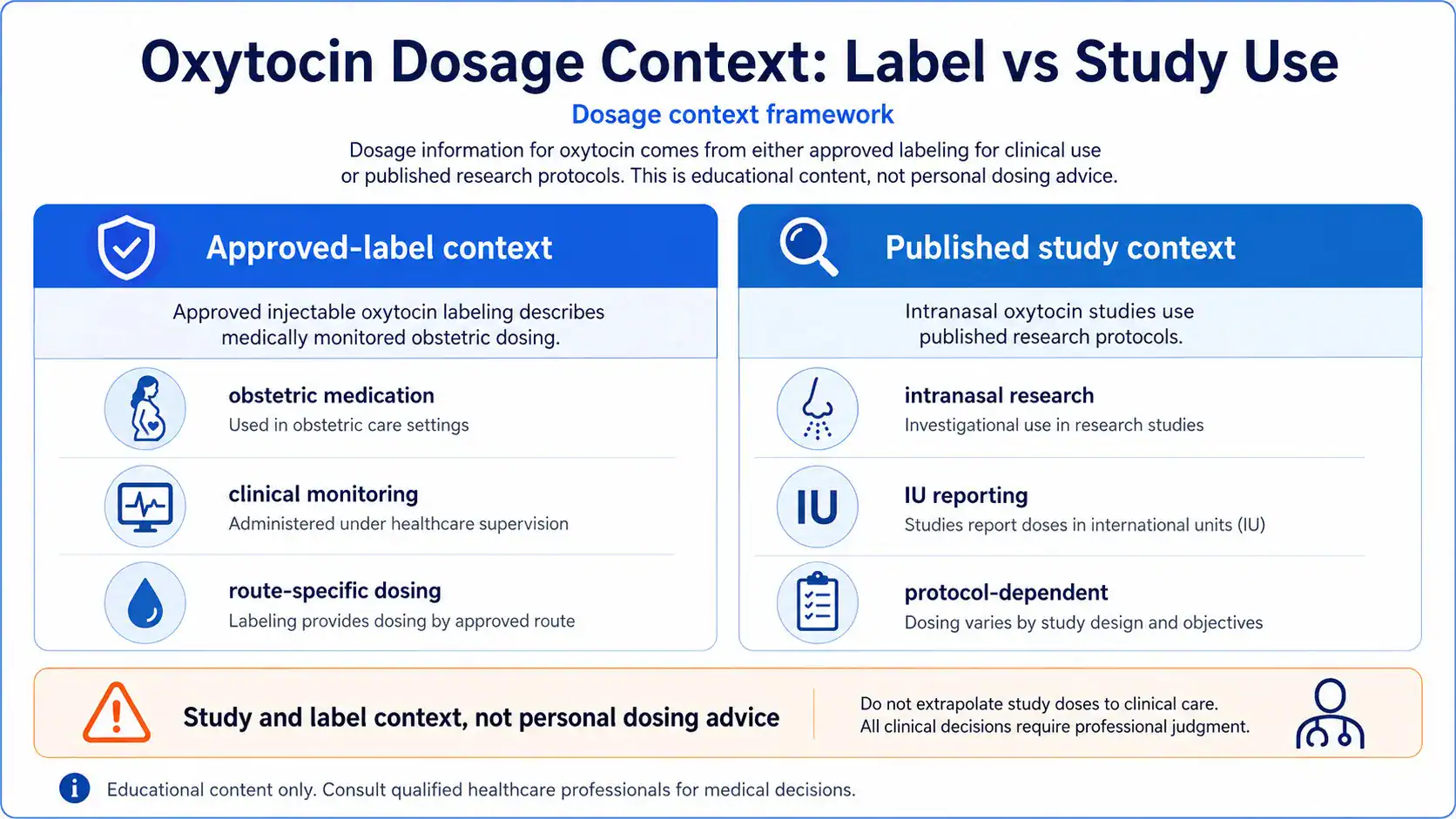
Oxytocin dosage information should be read as label or study context, not as a personal dose recommendation. Approved oxytocin dosing is individualized by uterine response and requires medical supervision, while intranasal study doses vary by trial [2], [5].
Approved-Label Dose Context for Medical Oxytocin
For labor induction or stimulation, Pitocin labeling states that the initial dose should be 0.5 to 1 mU/min, increased at 30 to 60 minute intervals by 1 to 2 mU/min until the desired contraction pattern is established [5]. Another DailyMed label states that the initial dose should be no more than 1 to 2 mU/min, with gradual increases of no more than 1 to 2 mU/min [2].
For postpartum uterine bleeding, DailyMed labeling describes 10 to 40 units added to 1,000 mL of nonhydrating diluent for IV infusion, or 10 units intramuscularly after delivery of the placenta [2]. These are hospital-use label contexts, not self-care instructions.
Studied Intranasal Oxytocin Doses and IU Reporting
Intranasal oxytocin studies commonly report doses in international units. The SOARS-B autism trial record describes dose escalation toward 24 IU twice daily, while the published pediatric ASD trial reported a target total daily dose of 48 IU [13], [10].
Other studies have used 12 IU twice daily, 24 IU/day, or 48 IU/day depending on age group, device, design, and study question [19], [16]. Because protocols differ, study dose does not equal a general therapeutic protocol.
Reconstitution and Concentration Concepts for Educational Context
Oxytocin concentration matters because labeled infusion dosing is based on units per volume and infusion rate. Pitocin labeling describes adding 10 units of oxytocin to 1,000 mL of 0.9% sodium chloride or Ringer’s lactate to yield 10 mU/mL in the infusion solution [5].
That example is included to explain how concentration appears in approved labeling. It should not be used as a home preparation guide, and oxytocin infusion requires clinical monitoring, infusion control, and immediate access to medical evaluation [5].
Administration Routes Discussed in Medical Literature
Oxytocin administration routes include intravenous infusion, intramuscular injection, and intranasal administration in research settings. Each route has different goals, risks, monitoring needs, and evidence strength [2], [4], [14].
Intravenous Oxytocin, Injection, and Clinical Monitoring
For induction or stimulation of labor, oxytocin injection labeling states that intravenous infusion is the acceptable method and that accurate control of infusion rate, uterine contraction monitoring, and fetal heart-rate monitoring are required [2], [5].
Intramuscular administration is described in postpartum contexts, including 10 units after delivery of the placenta in some labeling [2]. These routes belong to medical settings because excessive uterine stimulation, fetal distress, water intoxication, and other serious adverse events can occur [5].
Intranasal Administration of Oxytocin in Research Settings
Intranasal oxytocin administration is used mainly to study central oxytocin effects on brain and behavior. Reviews suggest intranasal administration can influence central oxytocin signaling, but debates remain about dose, device, delivery route, replication, and therapeutic translation [4].
Intranasal oxytocin should therefore be described as a research route for many behavioral indications, not as an approved or established treatment route for social enhancement, ASD, schizophrenia, or bonding outcomes [4], [10], [11].
Side Effects and Safety Concerns
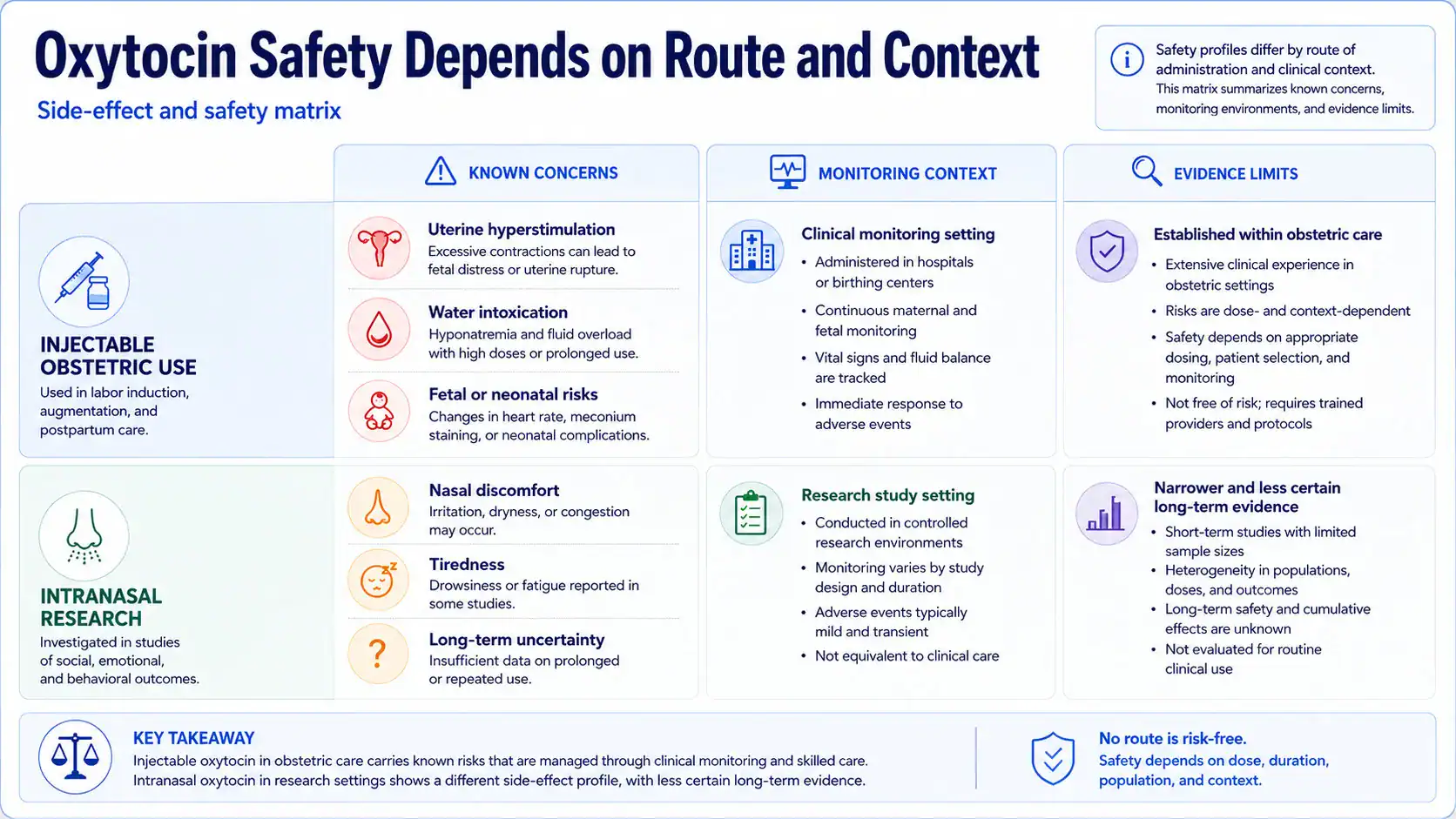
Oxytocin side effects and safety concerns depend on route, dose, indication, and monitoring. Parenteral oxytocin has serious obstetric risks when excessive uterine stimulation or overdose occurs, while intranasal studies usually report milder adverse events but have unresolved long-term questions [5], [11], 20.
Commonly Reported Side Effects by Route
Label-reported maternal adverse reactions include nausea, vomiting, cardiac arrhythmia, premature ventricular contractions, hypertensive episodes, postpartum hemorrhage, pelvic hematoma, anaphylactic reaction, subarachnoid hemorrhage, fatal afibrinogenemia, and uterine rupture [5]. Fetal or neonatal adverse reactions reported in labeling include bradycardia, low Apgar scores, arrhythmias, neonatal jaundice, neonatal retinal hemorrhage, permanent CNS or brain damage, and fetal death [5].
For intranasal oxytocin, a systematic review and meta-analysis reported common adverse events including nasal discomfort, tiredness, irritability, diarrhea, and skin irritation [20]. The pediatric NEJM trial reported similar incidence and severity of adverse events between oxytocin and placebo groups, but this does not prove safety for every population or long-term use [10].
Serious Risks in Pregnancy, Childbirth, and Uterine Stimulation
The most serious oxytocin risks occur in obstetric use when uterine activity becomes excessive or when contraindications are present. Labeling warns that excessive dosage or hypersensitivity may result in uterine hypertonicity, spasm, tetanic contraction, or rupture of the uterus [5].
Oxytocin can also have an antidiuretic effect. Labeling reports severe water intoxication with convulsions and coma after slow infusion over a 24-hour period and notes maternal death due to oxytocin-induced water intoxication [5].
Contraindications, Interactions, and Special Populations
Oxytocin contraindications and interactions are clinically important because oxytocin can affect both the mother and fetus in obstetric settings. Contraindications include situations where vaginal delivery is unsafe or where oxytocin may create excessive risk [2].
What Contraindications Should Be Reviewed Clinically?
DailyMed lists contraindications such as significant cephalopelvic disproportion, undeliverable fetal positions or presentations, obstetric emergencies favoring surgical intervention, fetal distress where delivery is not imminent, prolonged use in uterine inertia or severe toxemia, hypertonic uterine patterns, hypersensitivity, and induction or augmentation when vaginal delivery is contraindicated, including cord presentation or prolapse, total placenta previa, and vasa previa [2].
The label also cautions against use except in unusual circumstances in conditions such as prematurity, previous major cervical or uterine surgery including cesarean section, uterine overdistention, grand multiparity, and invasive cervical carcinoma [2].
Drug Interactions, Hormonal Context, and Medical Supervision
Oxytocin labeling reports severe hypertension when oxytocin was given three to four hours after prophylactic vasoconstrictor use with caudal block anesthesia [2]. Labeling also notes that cyclopropane anesthesia may modify cardiovascular effects and has been associated with maternal sinus bradycardia and abnormal atrioventricular rhythms when used with oxytocin [2].
Special populations require medical judgment. Labeling states that it is not known whether oxytocin is excreted in human milk and that caution should be exercised when oxytocin is administered to a nursing woman [2].
Regulatory Status of Oxytocin Peptide
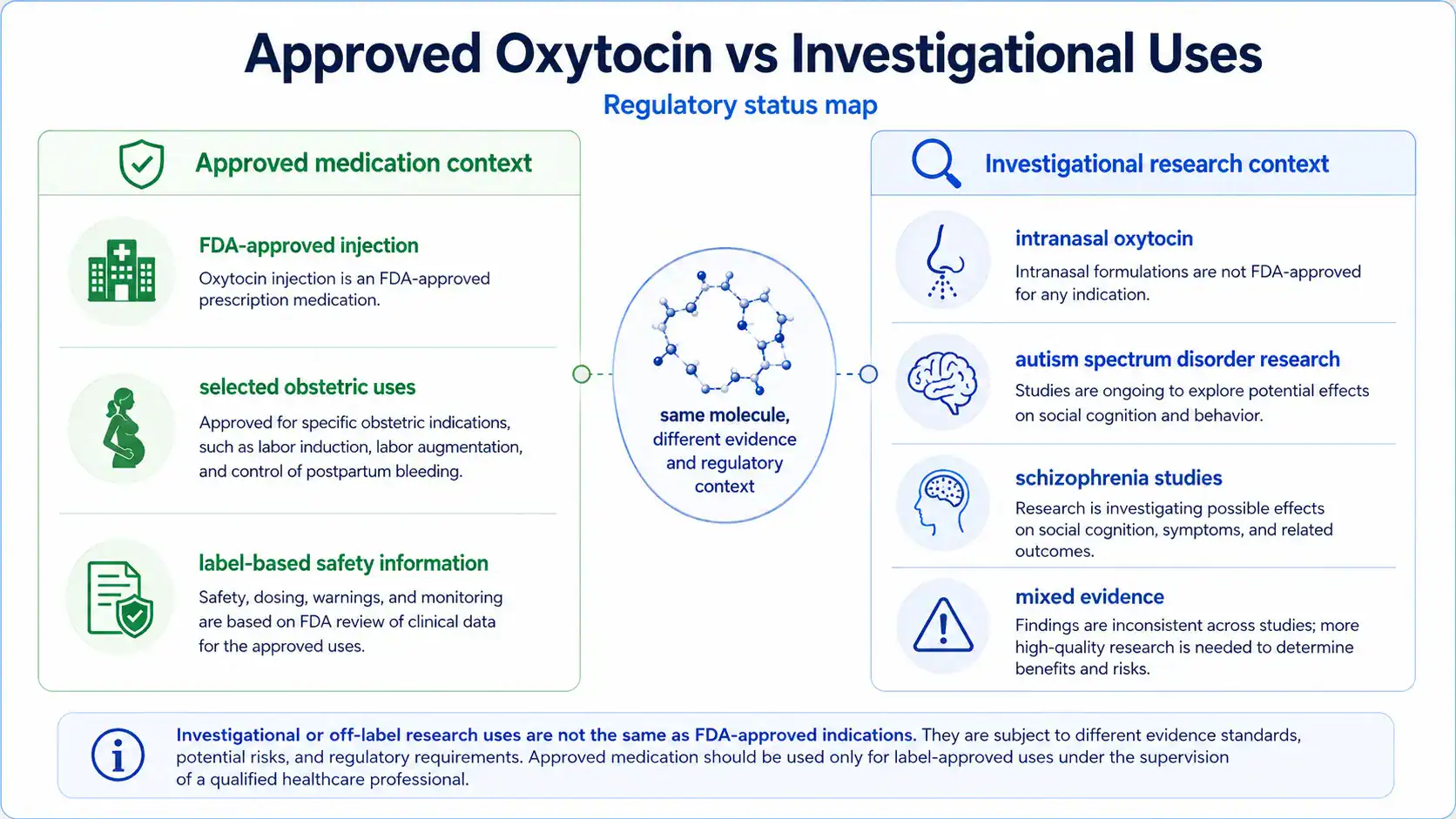
Oxytocin peptide has an approved prescription-drug status for certain injectable obstetric uses, while intranasal oxytocin for behavioral or psychiatric indications remains investigational or off-label depending on jurisdiction and product. Regulatory status determines what claims, dosing, quality controls, and safety labeling are established [2], [4].
FDA-Approved Oxytocin vs Investigational Intranasal Uses
DailyMed lists oxytocin injection as a human prescription drug label with approved medical indications and labeled dosing for selected antepartum and postpartum uses [2]. That approved status does not extend automatically to intranasal oxytocin nasal spray for autism spectrum disorder, schizophrenia, trust, social interaction, or relationship outcomes [4], [10], [11].
For research uses, ClinicalTrials.gov records and published trials can describe protocols, eligibility, dose ranges, and outcomes. They do not create approval for general personal use [13].
Evidence Limitations and Clinician Discussion Points
The safest interpretation of oxytocin peptide is to separate approved obstetric labeling from exploratory behavioral research and unsupported online claims. A clinician discussion should focus on indication, pregnancy status, contraindications, current medications, route, dose, regulatory status, and evidence quality [2], [4], [5].
Source Quality Checklist for Oxytocin Research
Use this checklist when evaluating oxytocin claims:
- Does the claim come from approved labeling, a regulator, a clinical guideline, a randomized trial, or a peer-reviewed review?
- Is the route clearly stated as intravenous, intramuscular, intranasal, endogenous release, or another route?
- Is the population clearly defined by age, sex, pregnancy status, diagnosis, and baseline characteristics?
- Are outcomes clinically meaningful, or are they laboratory measures such as gaze, emotion recognition, trust-game behavior, or fMRI activation?
- Does the source separate human evidence from animal or cell evidence?
- Does the claim avoid implying that a study dose is a personal protocol?
- Are contraindications, adverse events, and monitoring requirements discussed?
What Readers Should Discuss With a Qualified Clinician
Readers considering oxytocin-related medical decisions should discuss the reason for use, approved alternatives, pregnancy or breastfeeding status, obstetric history, cardiovascular risk, current medications, psychiatric diagnoses, and whether the proposed use is approved or investigational. For intranasal oxytocin, readers should also ask whether the evidence supports the specific condition, route, dose, device, duration, and outcome being considered [4], [10], [11].
The strongest conclusions about oxytocin peptide come from approved labeling and well-designed human studies. Claims based only on mechanism, animal models, online anecdotes, or single small trials should be treated cautiously.
REFERENCES
- National Center for Biotechnology Information. Oxytocin | PubChem Compound Summary. PubChem. Accessed 2026.
- DailyMed, U.S. National Library of Medicine. Oxytocin Injection, USP prescribing information. DailyMed drug label. Updated 2018.
- Patel H, et al. Physiology, Posterior Pituitary. StatPearls, NCBI Bookshelf. 2023.
- Quintana DS, Lischke A, Grace S, Scheele D, Ma Y, Becker B. Advances in the field of intranasal oxytocin research: lessons learned and future directions for clinical research. Molecular Psychiatry. 2021.
- DailyMed, U.S. National Library of Medicine. Pitocin, oxytocin injection prescribing information. DailyMed drug label.
- Hermesch AC, et al. Oxytocin: physiology, pharmacology, and clinical application. PubMed. 2024.
- Meyerowitz JG, et al. Oxytocin signaling complex reveals a molecular switch for cation dependence. Peer-reviewed article via PubMed Central. 2022.
- Kosfeld M, Heinrichs M, Zak PJ, Fischbacher U, Fehr E. Oxytocin increases trust in humans. Nature. 2005. PMID: 15931222.
- Domes G, Heinrichs M, Gläscher J, Büchel C, Braus DF, Herpertz SC. Oxytocin attenuates amygdala responses to emotional faces regardless of valence. Biological Psychiatry. 2007. PMID: 17617382.
- Sikich L, et al. Intranasal Oxytocin in Children and Adolescents with Autism Spectrum Disorder. New England Journal of Medicine. 2021. PMID: 34644471.
- Sabe M, et al. Intranasal Oxytocin for Negative Symptoms of Schizophrenia: Systematic Review and Dose-Response Meta-Analysis. PubMed. 2021.
- World Health Organization. Recommendations and supporting evidence: uterotonics for prevention of postpartum haemorrhage. NCBI Bookshelf / WHO recommendations.
- ClinicalTrials.gov. NCT01944046: Study of Oxytocin in Autism to Improve Reciprocal Social Behaviors. ClinicalTrials.gov registry.
- Martins DA, et al. Effects of route of administration on oxytocin-induced changes in regional cerebral blood flow in humans. Nature Communications. 2020.
- World Health Organization / NCBI Bookshelf. The physiological basis of breastfeeding. Infant and Young Child Feeding, NCBI Bookshelf.
- Yamasue H, et al. Effect of intranasal oxytocin on the core social symptoms of autism spectrum disorder: a randomized clinical trial. Molecular Psychiatry. 2020.
- Yamasue H, et al. Effect of a novel nasal oxytocin spray with enhanced bioavailability on autism spectrum disorder. PubMed. 2022.
- LoParo D, Waldman ID. The oxytocin receptor gene is associated with autism spectrum disorder: a meta-analysis. Molecular Psychiatry. 2015. PMID: 25092245.
- Daniels N, et al. Effects of multiple-dose intranasal oxytocin administration on social responsiveness in children with autism. Molecular Autism. 2023.
- Cai Q, et al. Systematic review and meta-analysis of reported adverse events of intranasal oxytocin. PubMed. 2018.
FAQs
What is oxytocin peptide and how does it work?
Oxytocin peptide is a naturally occurring peptide hormone and neuropeptide that also exists as a prescription medication for specific obstetric uses. It works mainly through the oxytocin receptor system, which helps regulate uterine contraction, milk-ejection physiology, and some central nervous system signaling pathways [1], [2], [3]. In research settings, oxytocin effects are also studied in social behavior, amygdala activity, trust, and emotional processing, but those findings do not prove broad therapeutic benefit [4].
What are oxytocin peptides used for?
Oxytocin peptides are used medically when approved oxytocin medication is clinically indicated, especially for selected labor induction, labor augmentation, and postpartum bleeding contexts [2]. Outside those approved uses, intranasal oxytocin treatment has been studied for autism spectrum disorder, schizophrenia, social interaction, trust, and related behavioral outcomes [4], [10], [11]. Those investigational uses remain evidence-sensitive because clinical findings are mixed and do not establish oxytocin as a general treatment for social or psychiatric conditions.
What are the potential health benefits of oxytocin peptide therapy?
Potential health benefits of oxytocin peptide therapy are strongest in approved obstetric settings, where oxytocin can support medically supervised uterine contraction and postpartum hemorrhage management [2], [12]. For social behavior, trust, empathy, mood, or bonding claims, the evidence is much less settled. Studies show that oxytocin may affect social processing, and one early study found that oxytocin increased trust in an experimental task, but this does not equal a proven therapy for daily-life outcomes [8].
Can oxytocin peptide help with anxiety, autism, schizophrenia, or mood disorders?
Oxytocin peptide has been studied in psychiatric and neurodevelopmental conditions, but it is not established as a reliable treatment for anxiety, autism, schizophrenia, or mood disorders. In autism spectrum disorder, larger trials have produced mixed or negative results, including a 24-week pediatric study that did not show significant social or cognitive benefit over placebo [10]. In schizophrenia, a meta-analysis found no consistent benefit for negative or positive symptoms [11]. These findings support caution rather than routine use.
How often should oxytocin peptide be taken, and what dosage information exists?
Oxytocin peptide dosage depends on whether the context is approved medical use or a published research protocol. Approved injectable oxytocin labeling describes carefully monitored infusion or intramuscular dosing in obstetric settings, such as labor induction or postpartum bleeding management [2], [5]. Intranasal studies have used research protocols such as 24 IU twice daily or 48 IU/day in autism trials [10], [13]. These are study or label contexts, not personal dosing recommendations.
Is oxytocin peptide safe, and what side effects can occur?
Oxytocin peptide safety depends on route, dose, indication, monitoring, pregnancy status, and medical history. Injectable oxytocin labeling reports serious risks, including uterine hyperstimulation, uterine rupture, water intoxication, cardiovascular effects, and fetal or neonatal adverse events when used improperly or in high-risk contexts [5]. Intranasal oxytocin studies more often report milder adverse events such as nasal discomfort, tiredness, irritability, diarrhea, or skin irritation, but long-term safety remains less certain [20].
Contributing Authors
The following authors are recognized for published research that helped shape the scientific and clinical context discussed in this article.
Daniel S. Quintana
Author profile: ORCID
Daniel S. Quintana is a published research author whose work is closely connected to intranasal oxytocin, neuropeptide research, and evidence quality in human behavioral studies. His publications are relevant to the article’s discussion of oxytocin peptide as a neuropeptide, the uncertainty around nose-to-brain delivery, the interpretation of social-cognition findings, and the need to distinguish mechanistic plausibility from clinical evidence. His work is especially useful for understanding why intranasal oxytocin research requires careful attention to study design, route of administration, reproducibility, dose context, and central versus peripheral effects.
Selected publications:
- Advances in the field of intranasal oxytocin research: lessons learned and future directions for clinical research — Molecular Psychiatry, 2021. DOI: 10.1038/s41380-020-00864-7
- Do delivery routes of intranasally administered oxytocin account for observed effects on social cognition and behavior? — Neuroscience & Biobehavioral Reviews, 2015. PMID: 25526824
Linmarie Sikich
Author profile: Duke Center for Autism and Brain Development
Linmarie Sikich is a clinical research author whose work is directly relevant to the article’s discussion of intranasal oxytocin, autism spectrum disorder, clinical study design, safety monitoring, and evidence limitations. Her publications help frame the difference between early interest in oxytocin for social functioning and the more cautious interpretation required after larger placebo-controlled research. This is particularly relevant for readers trying to understand oxytocin peptide beyond approved obstetric use, including why investigational findings in autism research should not be treated as general treatment recommendations.
Selected publications:
- Intranasal Oxytocin in Children and Adolescents with Autism Spectrum Disorder — New England Journal of Medicine, 2021. PMID: 34644471
- Rationale, design, and methods of the Autism Centers of Excellence network Study of Oxytocin in Autism to improve Reciprocal Social Behaviors — Contemporary Clinical Trials, 2020. PMID: 32777383
PUBLISHING FIELDS
- SEO Title: Oxytocin Peptide: Uses, Safety, Dosage and Research
- Meta Description: Oxytocin peptide guide covering approved uses, intranasal research, safety, side effects, dosage context, and evidence limits.
- Suggested URL Slug:
/oxytocin-peptide - Page Type: Therapeutic Peptide Educational Article
- ArticleFormat: Therapeutic Peptide Educational Guide
- TargetPeptide: Oxytocin
- MainKeyword: oxytocin peptide
- CanonicalKeyword: oxytocin peptide
- ExactKeywordVariant: Same as CanonicalKeyword
- AliasTerms: oxytocin, oxytocin peptide hormone, peptide hormone, endogenous oxytocin, intranasal oxytocin, oxytocin nasal spray, oxytocin medication
- PeptideCategory: Approved Peptide Drug / Neuropeptide / Peptide Hormone
- Primary Search Intent: Therapeutic informational
- Secondary Keywords: intranasal oxytocin, oxytocin nasal spray, oxytocin receptor, oxytocin hormone, oxytocin medication, oxytocin dosage, oxytocin side effects, oxytocin safety, oxytocin research, oxytocin and autism spectrum disorder, oxytocin treatment, oxytocin benefits
- Evidence Levels Covered: approved medical use, clinical evidence, early human evidence, preclinical evidence, unsupported or mixed claims
- Excerpt: Oxytocin peptide is a naturally occurring peptide hormone and approved prescription medication for selected obstetric uses. This educational guide reviews how oxytocin works, approved and investigational uses, intranasal oxytocin research, dosage context, safety concerns, side effects, contraindications, regulatory status, and evidence limitations.
- Suggested Tags: oxytocin, oxytocin peptide, neuropeptides, peptide hormones, intranasal oxytocin, peptide safety, clinical evidence, FDA-approved peptide drugs
- Featured Image Concept: Clinical evidence map showing oxytocin as an endogenous peptide hormone, approved obstetric medication, and investigational intranasal research topic.
- Featured Image Alt Text: Oxytocin peptide evidence map showing approved uses, intranasal research, safety, and dosage context.
- Suggested Schema: Article schema only.
INFOGRAPHIC BRIEFS
Infographic Brief 1
- Placement:
## How Does Oxytocin Peptide Work? - Title: How Oxytocin Peptide Signals Through the Body
- Purpose: Explain the difference between oxytocin receptor signaling in peripheral tissues and oxytocin’s studied central nervous system effects.
- Visual Format: Mechanism of action diagram
- Key Labels: Oxytocin peptide, oxytocin receptor, hypothalamus, posterior pituitary, uterus, breast tissue, central nervous system, social-cognition research
- Suggested Layout: A left-to-right pathway diagram beginning with hypothalamic production, moving to posterior pituitary release, then branching into peripheral effects and CNS research pathways.
- Data or Concepts to Include: Oxytocin is produced in the hypothalamus, released through the posterior pituitary, binds the oxytocin receptor, supports uterine contraction and milk-ejection physiology, and is studied for central signaling and social behavior.
- Visual Style: Clean clinical illustration with simple labeled nodes, soft anatomical silhouettes, and no decorative clutter.
- Compliance Restrictions: Do not show syringes, self-administration, dosing instructions, product packaging, or guaranteed behavioral effects.
- Alt Text: Mechanism diagram showing how oxytocin peptide interacts with oxytocin receptors in peripheral tissues and central nervous system research pathways.
- Full AI Image Prompt: Create a clean clinical infographic titled “How Oxytocin Peptide Signals Through the Body.” Show a simplified hypothalamus and posterior pituitary on the left, with arrows leading to two branches: peripheral effects and central nervous system research. The peripheral branch should include labeled icons for uterus and breast tissue with labels “uterine contraction” and “milk-ejection physiology.” The CNS research branch should include a simplified brain circuit icon labeled “social-cognition research” and “central signaling.” Include labels for “oxytocin peptide” and “oxytocin receptor.” Use a professional medical editorial style, soft neutral colors, clear typography, and no syringe imagery, product packaging, dosing steps, or outcome promises.
Infographic Brief 2
- Placement:
## What Does Human Research Show About Oxytocin? - Title: Oxytocin Evidence by Research Area
- Purpose: Help readers distinguish approved medical use from clinical, early human, preclinical, and unsupported or mixed claims.
- Visual Format: Evidence ladder or evidence matrix
- Key Labels: Approved obstetric use, postpartum bleeding context, intranasal oxytocin, autism spectrum disorder, schizophrenia, trust research, preclinical models, evidence limitations
- Suggested Layout: A vertical evidence ladder with the strongest evidence at the top and weaker or more uncertain categories lower down.
- Data or Concepts to Include: Approved obstetric use is the strongest evidence category; intranasal oxytocin research for autism spectrum disorder and schizophrenia is mixed; trust and social-cognition findings are early human or experimental; animal and mechanism studies have translational limits.
- Visual Style: Editorial evidence graphic with neutral colors, restrained icons, and clear evidence-level labels.
- Compliance Restrictions: Do not imply oxytocin treats autism, schizophrenia, anxiety, mood disorders, or social outcomes. Do not use checkmarks that imply proven benefits for investigational uses.
- Alt Text: Oxytocin peptide evidence ladder comparing approved medical use, clinical research, early human findings, and preclinical evidence.
- Full AI Image Prompt: Create a medically responsible evidence ladder infographic titled “Oxytocin Evidence by Research Area.” Use four stacked levels: “Approved Medical Use,” “Clinical Evidence,” “Early Human Evidence,” and “Preclinical or Mechanistic Evidence.” Under Approved Medical Use, include “selected obstetric uses” and “postpartum bleeding context.” Under Clinical Evidence, include “intranasal oxytocin in autism spectrum disorder” and “schizophrenia studies” with a label “mixed findings.” Under Early Human Evidence, include “trust and social-cognition tasks.” Under Preclinical or Mechanistic Evidence, include “animal models” and “brain-circuit research.” Use a clean clinical design, avoid promotional language, avoid benefit guarantees, and do not include product or injection imagery.
Infographic Brief 3
- Placement:
## Oxytocin Dosage Information From Labels and Published Studies - Title: Oxytocin Dosage Context: Label vs Study Use
- Purpose: Clarify that dosage information in the article comes from approved labeling or published study protocols, not personal dosing advice.
- Visual Format: Dosage context framework
- Key Labels: Approved-label dosing, study protocol doses, IU reporting, route matters, clinical monitoring, not personal advice
- Suggested Layout: Two-column comparison showing “Approved-label context” and “Published study context,” with a caution band beneath both columns.
- Data or Concepts to Include: Approved injectable oxytocin labeling describes medically monitored obstetric dosing; intranasal studies have used IU-based research protocols; route, dose, timing, and monitoring change interpretation.
- Visual Style: Clean educational framework with restrained medical icons and clear caution language.
- Compliance Restrictions: Do not create a dosing chart that looks like a personal protocol. Do not include step-by-step administration, self-injection, reconstitution tutorials, or “best dose” language.
- Alt Text: Oxytocin peptide dosage context infographic comparing approved-label dosing and published intranasal study protocols.
- Full AI Image Prompt: Create a clinical educational infographic titled “Oxytocin Dosage Context: Label vs Study Use.” Use two side-by-side columns. The left column is labeled “Approved-label context” and includes short labels: “obstetric medication,” “clinical monitoring,” “route-specific dosing.” The right column is labeled “Published study context” and includes short labels: “intranasal research,” “IU reporting,” “protocol-dependent.” Add a bottom caution band reading “Study and label context, not personal dosing advice.” Use clean editorial typography, neutral colors, no syringe-focused imagery, no step-by-step dosing instructions, no reconstitution tutorial, and no product packaging.
Infographic Brief 4
- Placement:
## Side Effects and Safety Concerns - Title: Oxytocin Safety Depends on Route and Context
- Purpose: Show that safety risks differ between injectable obstetric use and intranasal research settings.
- Visual Format: Side-effect and safety matrix
- Key Labels: Injectable oxytocin, intranasal oxytocin, uterine hyperstimulation, water intoxication, fetal or neonatal risks, nasal discomfort, tiredness, long-term uncertainty
- Suggested Layout: A matrix with rows for “Injectable obstetric use” and “Intranasal research,” and columns for “Known concerns,” “Monitoring context,” and “Evidence limits.”
- Data or Concepts to Include: Injectable oxytocin labeling includes serious obstetric risks; intranasal oxytocin studies more often report milder adverse events but long-term safety remains less certain.
- Visual Style: Clinical safety graphic with caution icons and muted colors.
- Compliance Restrictions: Do not imply any form is safe for everyone. Do not show emergency imagery, fear-based visuals, product branding, or self-use instructions.
- Alt Text: Oxytocin peptide safety matrix comparing injectable obstetric risks with intranasal oxytocin research safety considerations.
- Full AI Image Prompt: Create a clean clinical safety matrix titled “Oxytocin Safety Depends on Route and Context.” Include two rows: “Injectable obstetric use” and “Intranasal research.” Include three columns: “Known concerns,” “Monitoring context,” and “Evidence limits.” For injectable use, include labels such as “uterine hyperstimulation,” “water intoxication,” and “fetal or neonatal risks.” For intranasal research, include labels such as “nasal discomfort,” “tiredness,” and “long-term uncertainty.” Use restrained caution icons, professional medical colors, and clear typography. Avoid self-administration imagery, product packaging, fear-based visuals, or claims of guaranteed safety.
Infographic Brief 5
- Placement:
## Regulatory Status of Oxytocin Peptide - Title: Approved Oxytocin vs Investigational Uses
- Purpose: Explain the article’s key regulatory distinction between approved injectable oxytocin medication and investigational intranasal or behavioral research uses.
- Visual Format: Approved vs investigational status map
- Key Labels: FDA-approved injection, obstetric indications, investigational intranasal research, autism spectrum disorder research, schizophrenia studies, off-label context, evidence quality, clinician discussion
- Suggested Layout: A split map with “Approved medication context” on one side and “Investigational research context” on the other, joined by a center label: “same molecule, different evidence and regulatory context.”
- Data or Concepts to Include: Oxytocin injection has approved prescription-drug labeling for selected obstetric uses; intranasal oxytocin for behavioral and psychiatric indications remains investigational or off-label depending on context.
- Visual Style: Professional regulatory explainer with a balanced, neutral layout.
- Compliance Restrictions: Do not imply investigational uses are approved. Do not include buying guidance, vendor language, product images, or personal-use recommendations.
- Alt Text: Oxytocin peptide regulatory status map distinguishing approved injectable medication from investigational intranasal research uses.
- Full AI Image Prompt: Create a professional regulatory infographic titled “Approved Oxytocin vs Investigational Uses.” Use a split-panel design. Left panel: “Approved medication context” with labels “FDA-approved injection,” “selected obstetric uses,” and “label-based safety information.” Right panel: “Investigational research context” with labels “intranasal oxytocin,” “autism spectrum disorder research,” “schizophrenia studies,” and “mixed evidence.” Add a central connector label reading “same molecule, different evidence and regulatory context.” Use a clean medical editorial style, neutral colors, no product packaging, no purchase language, no syringe-focused visuals, and no treatment promises.