IGF-1 DES peptide is a truncated form of insulin-like growth factor 1 that appears in scientific literature as des(1-3)IGF-I, IGF-1 Des(1–3), or IGF-1(4–70) 1. This educational article reviews what is known about IGF-1 DES, what is extrapolated from broader IGF-1 research, and where online claims about muscle growth, bodybuilding, dosage, and target muscle effects go beyond reliable evidence. It does not provide personalized medical advice or instructions for self-use.
- IGF-1 DES is an N-terminally truncated IGF-1 variant missing the first three amino acids found in native IGF-1 [1].
- The main scientific interest is that IGF-1 DES has reduced binding to IGF-binding proteins, which can make it more bioactive in some cell and animal models [1], 3.
- IGF-1 DES is discussed online for muscle growth, hypertrophy, target muscle effects, and bodybuilding, but those claims are not supported by strong human clinical evidence.
- Human medical approval applies to mecasermin, a recombinant human IGF-1 drug, not to IGF-1 DES 13.
- Safety concerns are biologically plausible because IGF-1 signaling affects glucose handling, cell growth, tissue growth, and receptor pathways involved in proliferation 11, [13].
- Published dosage context for IGF-1 DES comes mainly from preclinical studies; online “protocol” ranges should not be treated as evidence-based dosing.
- Regulatory status matters: IGF-1 DES is not an FDA-approved peptide drug, and IGF-1 and analogues are also relevant to anti-doping rules in sport 18.
Fast Answer
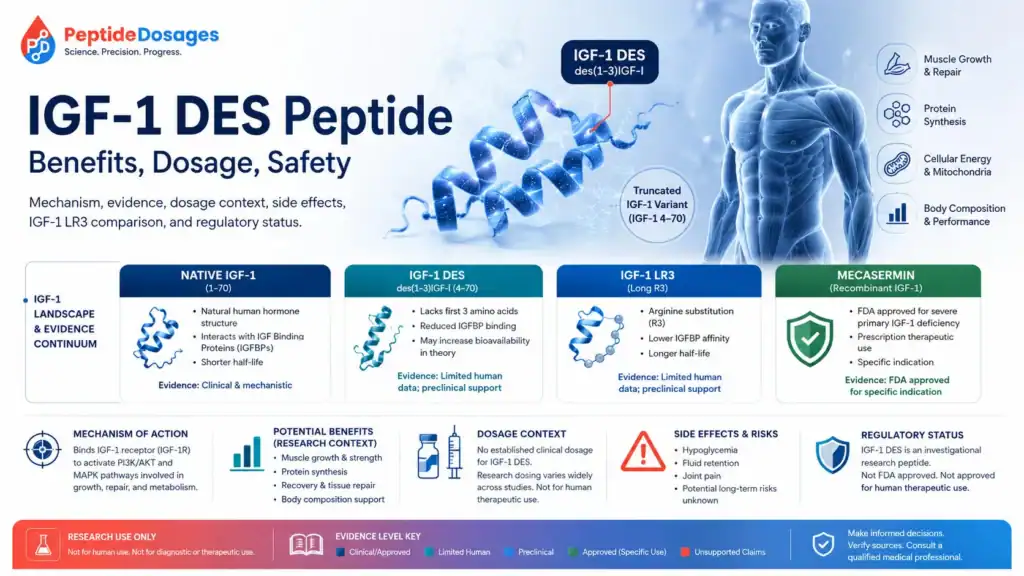
IGF-1 DES peptide is an investigational IGF-1 variant, not an FDA-approved therapy. It is a truncated form of insulin-like growth factor 1 that has been studied mainly because it binds poorly to IGF-binding proteins and can show stronger activity than native IGF-1 in some laboratory and animal models [1], [3]. Searches often focus on muscle growth, hypertrophy, and bodybuilding, but reliable human evidence for IGF-1 DES use, dosage, safety, or benefits is limited.
Evidence basis note: This page prioritizes regulator labeling, peer-reviewed studies, biomedical databases, clinical-trial records, and scientific reviews. Claims that appear mainly in bodybuilding or peptide-marketing content are treated as unverified unless they are supported by reliable published evidence.
What Is the IGF-1 DES Peptide?
IGF-1 DES peptide is a shortened insulin-like growth factor 1 variant that lacks the first three amino acids at the N-terminus of native IGF-1 [1]. In scientific writing, the same molecule is commonly called des(1-3)IGF-I or IGF-1(4–70), which helps distinguish it from native IGF-1 and longer engineered analogues such as IGF-1 LR3 [1], 2.
IGF-1 DES as a Truncated Form of Insulin-Like Growth Factor 1
IGF-1 DES is a truncated form of insulin-like growth factor 1, a peptide hormone involved in growth, metabolism, and cellular signaling [1], [2]. Native IGF-1 is a 70-amino-acid protein, while IGF-1 DES is described as a 67-amino-acid variant missing the Gly-Pro-Glu tripeptide from the N-terminus [1].
That structural difference is small on paper but important biologically. IGF-binding proteins strongly regulate native IGF-1 activity in blood and tissues, and reduced binding can change how much peptide is available to interact with receptors [2], [11].
The Role of the N-Terminus and First Three Amino Acids
The N-terminus matters because the absence of the first three amino acids changes IGF-1 DES interaction with IGF-binding proteins [1]. Ballard and colleagues reported that the missing N-terminal tripeptide, especially the absence of glutamate at position 3, contributes to reduced IGF-binding protein affinity and higher activity in some cultured-cell systems [1].
This does not mean IGF-1 DES has proven therapeutic superiority in humans. It means the structural change creates a mechanistic rationale for why researchers have studied its potency, bioavailability, localized effects, and systemic effects.
Why IGF-1 DES Is Discussed as an Investigational Growth Factor Peptide
IGF-1 DES is discussed as an investigational growth factor peptide because it belongs to the IGF signaling family but is not an approved drug for a labeled medical indication. By contrast, mecasermin is an FDA-approved recombinant human IGF-1 product for specific pediatric growth-failure indications in severe primary IGF-1 deficiency or growth hormone gene deletion with neutralizing antibodies to growth hormone [13].
The distinction matters. A molecule can be biologically related to an approved drug without being approved, interchangeable, or clinically validated for the same uses.
IGF-1 DES, Native IGF-1, and IGF-1 LR3 Explained
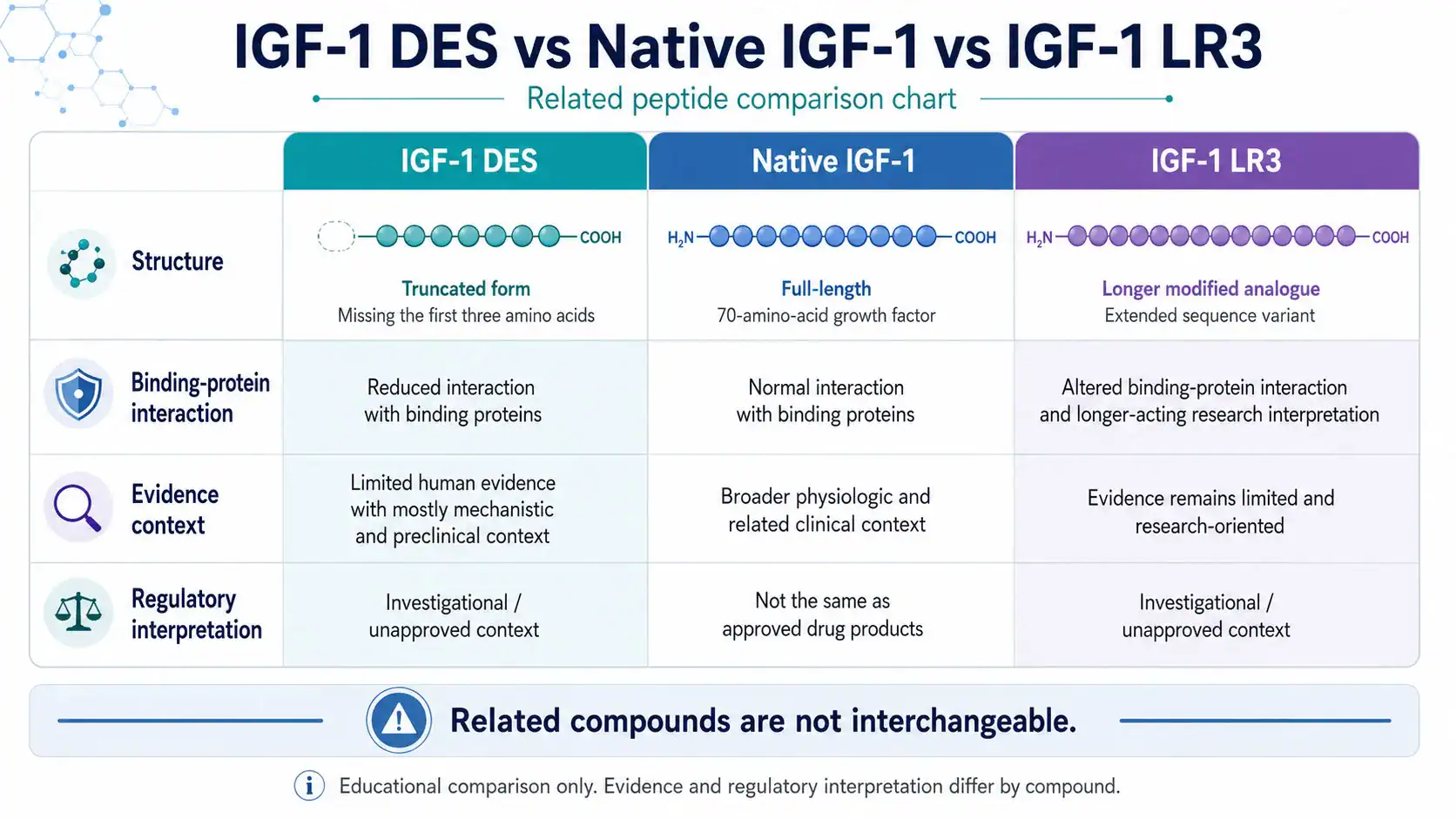
IGF-1 DES, native IGF-1, and IGF-1 LR3 all relate to insulin-like growth factor biology, but they differ in structure, binding-protein interaction, duration, and evidence quality. The article should treat them as related but separate compounds, not as interchangeable names for the same peptide.
How IGF-1 DES Differs From Native IGF-1
Native IGF-1 is the full-length 70-amino-acid growth factor regulated by growth hormone, IGF-binding proteins, receptors, tissues, nutrition, and endocrine feedback [2], [11]. IGF-1 DES is shortened at the N-terminus and shows reduced binding to IGF-binding proteins compared with native IGF-1 in multiple experimental systems [1], [3], 4.
In one classic biochemical study, IGF-binding proteins inhibited the biological activities of IGF-1 and IGF-2 but did not inhibit des(1-3)IGF-1 in the same way [3]. That finding supports the mechanistic idea of greater free or local activity, but it still comes from experimental systems rather than therapeutic trials in people.
IGF-1 LR3 vs IGF-1 DES: Key Structural and Functional Differences
IGF-1 LR3 and IGF-1 DES are both modified IGF-1 variants, but they are modified differently. IGF-1 DES is N-terminally truncated, while IGF-1 LR3 is commonly described as a long arginine-3 IGF-1 analogue with a longer extension and reduced binding-protein interaction [2], 5.
The practical SEO issue is that “IGF-1 LR3 vs IGF-1 DES” searches often come from bodybuilding or performance-enhancement contexts. A medical article should answer the comparison by focusing on structure, receptor biology, evidence level, regulatory status, and safety uncertainty, not by recommending which one is “best.”
Why IGF-1 Variants Should Not Be Treated as Interchangeable
IGF-1 variants should not be treated as interchangeable because small sequence changes can alter receptor binding, binding-protein affinity, pharmacokinetics, tissue exposure, and safety behavior [5], 6. In animal research, variants that bind poorly to IGF-binding proteins showed more potent and prolonged glucose-lowering effects than native IGF-1 [6].
That glucose signal is especially important for safety interpretation. A more “potent” growth factor effect in a model can also mean a higher or less predictable risk of systemic metabolic effects.
How Does IGF-1 DES Peptide Work?
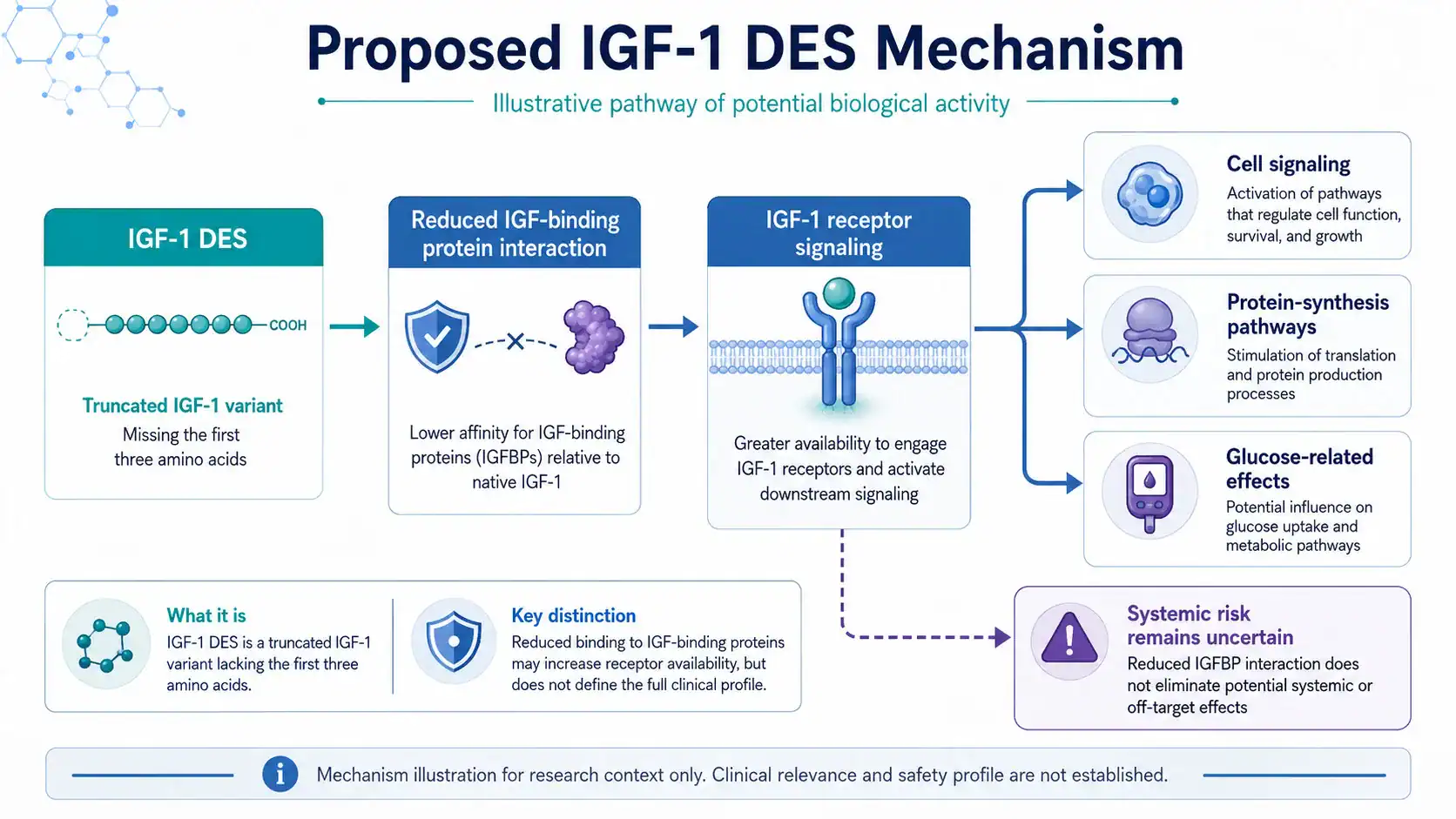
IGF-1 DES peptide is thought to work through IGF-1 receptor signaling while showing reduced interaction with IGF-binding proteins compared with native IGF-1 [1], [3]. The proposed mechanism centers on receptor activation, cell signaling, protein biosynthesis, and tissue-growth pathways, but clinical outcomes in humans remain unproven.
IGF-1 Receptor Binding and Cell Signaling
The IGF-1 receptor is a receptor tyrosine kinase related to the insulin receptor, and activation of this receptor can trigger intracellular signaling pathways involved in growth, survival, differentiation, and metabolism 12. FDA labeling for mecasermin describes IGF-1 receptor activation as part of the mechanism leading to statural growth and metabolic actions such as glucose uptake [13].
IGF-1 DES appears to preserve receptor activity while being less constrained by certain binding proteins [1], [4]. That is the core reason researchers discuss it as a potent IGF-related peptide.
Growth Factor Binding Proteins and Local Activity
IGF-binding proteins regulate IGF access to receptors, tissue distribution, half-life, and bioavailability [11]. A 2021 review noted that IGFBPs bind a large proportion of circulating IGF-1 and play a major role in controlling IGF function [2].
Because IGF-1 DES has reduced affinity for IGF-binding proteins, it may show stronger local effects in some cell systems [1], [3]. The phrase “localized effects,” however, should not be turned into a clinical claim that a target muscle can be selectively enlarged in humans.
Short Half-Life, Localized Effects, and Systemic Effects
IGF-1 DES is commonly described as having a short half-life compared with some engineered IGF-1 analogues, but exact human pharmacokinetic data for IGF-1 DES are not well established in reliable clinical sources. Broader IGF-1 pharmacokinetics cannot be directly applied to IGF-1 DES because binding-protein interaction is part of what determines distribution and clearance [11], [13].
The key practical point is simple: reduced binding-protein interaction may increase local bioactivity, but it does not remove systemic risk. IGF-related compounds can still affect glucose, insulin-like signaling, tissue growth, and cell proliferation pathways [6], [13].
Mechanism of Action: Muscle Cells, Satellite Cells, and Protein Biosynthesis
The muscle-related mechanism proposed for IGF-1 DES is based on broader IGF-1 biology: IGF-1 signaling is involved in skeletal muscle protein synthesis, satellite cell activity, hypertrophy, and the balance between anabolic and catabolic pathways 10. Evidence specific to IGF-1 DES is strongest in preclinical and mechanistic contexts, not in human outcome trials.
Effects on Muscle Cell Growth and Differentiation
IGF-1 signaling affects muscle cell growth and differentiation through pathways that include PI3K/Akt and related protein-synthesis signaling [10]. In cultured-cell and animal research, des(1-3)IGF-I has shown stronger biological activity than native IGF-1 in some settings, which researchers have linked to reduced binding-protein inhibition [1], [3].
That is why IGF-1 DES appears in discussions of muscle hypertrophy. The evidence supports biological plausibility, not a validated human treatment for muscle growth.
Satellite Cell and Myosatellite Cell Research
Satellite cells are muscle-resident precursor cells involved in repair, adaptation, and growth responses. Reviews of IGF-1 in skeletal muscle describe IGF-1 as a regulator of muscle hypertrophy, muscle regeneration, and satellite-cell-related pathways [10].
The IGF-1 DES leap is more cautious. Because IGF-1 DES is an IGF-1 variant, its research relevance overlaps with these pathways, but direct human studies proving satellite-cell benefit from IGF-1 DES are lacking.
Muscle Protein Synthesis, Hypertrophy, and Anabolic Signaling
IGF-1 is part of the endocrine and local signaling network that can influence muscle protein synthesis and skeletal muscle hypertrophy [10]. Local infusion of IGF-1 in a rat muscle model increased the absolute weight of the infused tibialis anterior muscle by about 9% and increased protein and DNA content, suggesting direct muscle effects in that preclinical setting 19.
That study involved IGF-1 in rats, not IGF-1 DES in humans. It is useful for understanding mechanism, but it should not be interpreted as evidence for bodybuilding outcomes.
What Is IGF-1 DES Peptide Used For or Studied For?
IGF-1 DES peptide has been studied mainly as a research tool for IGF biology, binding-protein interaction, tissue growth, and preclinical anabolic effects. It does not have the same approved medical use as mecasermin, and therapeutic claims should be separated from online or anecdotal claims.
Skeletal Muscle and Muscle Hypertrophy Research
Skeletal muscle research around IGF-1 focuses on hypertrophy, atrophy, protein turnover, satellite cells, and muscle regeneration [10]. IGF-1 DES enters this topic because it can show increased potency in experimental models compared with native IGF-1 [1], 9.
The strongest language supported by the literature is that IGF-1 DES has been explored in preclinical systems relevant to muscle growth and anabolic signaling. It is not accurate to say that IGF-1 DES is proven to increase lean muscle in humans.
Tissue Growth, Injury Models, and Recovery Questions
IGF-1 DES has also appeared in animal models involving growth and tissue repair. In rats after extensive small-bowel resection, IGF-I and des(1-3)IGF-I were administered by osmotic infusion pumps over 7 days, with dosing reported as 0.96 mg/kg/day for des(1-3)IGF-I in that model 7.
Another rat model examined IGF-I and des(1-3)IGF-I in renal insufficiency, reporting effects on somatic growth and nitrogen balance 8. These studies support preclinical interest in tissue growth and recovery, but they do not establish a human recovery protocol.
Metabolic, Glucose, and Insulin-Like Effects Under Study
IGF-related peptides can affect carbohydrate metabolism because IGF-1 has insulin-like effects on glucose uptake and peripheral glucose utilization [13]. FDA labeling for mecasermin specifically warns about severe hypoglycemia, including hypoglycemic seizures, because of insulin-like hypoglycemic effects [13].
Animal research on IGF-I variants that bind poorly to IGF-binding proteins found more potent and prolonged hypoglycemic action than native IGF-I in pigs and marmoset monkeys [6]. That finding is not a benefit claim; it is a safety signal that should make glucose-related risk part of any serious discussion.
Potential Benefits of IGF-1 DES Peptide
Potential benefits of IGF-1 DES peptide are best described as evidence-graded hypotheses: stronger laboratory activity, preclinical tissue-growth effects, and mechanistic relevance to muscle and metabolism. Human therapeutic benefits remain unconfirmed for IGF-1 DES itself.
| Evidence Area | What Has Been Studied | Evidence Level | What It Can and Cannot Show |
|---|---|---|---|
| IGF-binding protein interaction | IGF-binding proteins inhibited IGF-1 and IGF-2 activity but not des(1-3)IGF-1 in a classic biochemical model [3] | Preclinical / mechanistic | Shows altered binding-protein regulation, not human efficacy |
| Potency in cell systems | Des(1-3)IGF-I was reported as about 10-fold more potent than IGF-I in stimulating hypertrophy and proliferation of cultured cells [1] | Preclinical / in vitro | Supports potency hypothesis, not a clinical dose or outcome |
| Animal growth models | IGF-I and des(1-3)IGF-I enhanced growth in rat models after surgery or renal insufficiency [7], [8] | Preclinical animal | Shows biological activity in animals, not therapeutic benefit in humans |
| Glucose effects | Poorly IGFBP-binding IGF-I variants showed stronger glucose-lowering effects than native IGF-I in animal models [6] | Preclinical animal | Indicates possible systemic risk, not a safe metabolic benefit |
| Approved IGF-1 therapy context | Mecasermin is approved for specific pediatric severe primary IGF-1 deficiency indications [13], 14 | Approved medical use for mecasermin only | Does not validate IGF-1 DES as an approved therapy |
Muscle Growth and Recovery Claims
Muscle growth and recovery claims around IGF-1 DES are usually based on a chain of reasoning: IGF-1 affects muscle biology, IGF-1 DES can be more bioactive in some models, and online users extrapolate that to hypertrophy or recovery. The first two ideas have scientific support in specific contexts [1], [10]. The third is not established clinical evidence.
A responsible benefits section should say that IGF-1 DES is relevant to muscle-growth research. It should not claim guaranteed gains with IGF-1, new muscle formation, or improved performance in humans.
Target Muscle Effects: What the Hypothesis Suggests
The “target muscle” idea is usually tied to the concept that shorter-acting or less binding-protein-bound IGF variants might act locally at the site of exposure. Preclinical IGF-1 infusion research supports the possibility that local IGF signaling can affect muscle size and protein content in rats [19].
The evidence does not prove that IGF-1 DES can be used to selectively enlarge a chosen muscle group in humans. Target muscle claims remain largely speculative when presented as practical bodybuilding guidance.
What Benefits Remain Theoretical or Preclinical
Theoretical or preclinical benefit claims include muscle hypertrophy, localized anabolic effects, tissue growth, recovery, and altered metabolic signaling. These topics are scientifically relevant, but they remain limited by model type, dose differences, species differences, and lack of well-designed human trials specific to IGF-1 DES [1], [7], [8].
The evidence is strongest for mechanism. It is weakest for human outcomes.
IGF-1 DES for Bodybuilding: Claims vs Evidence
IGF-1 DES for bodybuilding is a high-risk search topic because online claims often treat experimental growth-factor biology as if it were a validated performance-enhancement protocol. Published evidence does not support presenting IGF-1 DES as a proven bodybuilding peptide.
Why Bodybuilding Searches Focus on Hypertrophy and Lean Muscle
Bodybuilding searches focus on hypertrophy, lean muscle, satellite cells, muscle group targeting, and anabolic effects because IGF-1 biology overlaps with muscle growth pathways [10]. IGF-1 DES adds another layer because it has reduced IGF-binding protein interaction and higher activity in some preclinical models [1], [3].
That overlap explains the search interest. It does not establish safety, legality, dosing, or human efficacy.
Gains With IGF-1: What Online Claims Often Overstate
Online claims often overstate “gains with IGF-1” by skipping the difference between native IGF-1, IGF-1 DES, IGF-1 LR3, mecasermin, and endogenous IGF-1 signaling. Mecasermin is a regulated drug for rare pediatric growth-failure indications, while IGF-1 DES is not approved for bodybuilding, muscle gain, or recovery [13], [14].
The strongest evidence for IGF-1 DES remains preclinical. That should be the main frame for readers.
Performance-Enhancement Claims and Medical Caution
Performance-enhancement claims require medical and regulatory caution. The World Anti-Doping Agency’s Prohibited List includes insulin-like growth factor 1 and analogues under prohibited peptide hormones, growth factors, related substances, and mimetics [18].
That anti-doping status is separate from medical safety, but it underscores why bodybuilding-oriented use is not a neutral wellness topic. It involves regulated growth-factor biology with real safety concerns.
What Does Human Research Show About IGF-1 DES?
Human research specifically on IGF-1 DES is limited, and much of the discussion relies on broader IGF-1 biology, approved mecasermin labeling, and preclinical IGF-1 DES studies. Readers should not treat mecasermin data or native IGF-1 data as proof that IGF-1 DES is safe or effective.
Human Evidence for IGF-1 DES Specifically
The available literature map for IGF-1 DES is dominated by biochemical, cell, review, and animal-model studies rather than large human clinical trials [1], [3], [7], [8]. That evidence can explain mechanism and biological plausibility, but it cannot define human dosage, long-term safety, therapeutic benefits, or adverse-event rates.
This is the central evidence limitation for IGF-1 DES peptide. Human claims should be treated cautiously unless they are tied to direct human data.
What Broader IGF-1 Research Can and Cannot Explain
Broader IGF-1 research can explain the IGF axis, receptor biology, growth hormone connection, binding proteins, glucose effects, and why IGF signaling matters in muscle, growth, and metabolism [2], [11], [12]. Broader IGF-1 research cannot automatically answer whether IGF-1 DES has the same pharmacokinetics, safety profile, tissue exposure, or clinical effect.
A close analogy is useful but not conclusive. For peptide variants, structural differences are often the whole point.
Why Approved IGF-1 Therapy Does Not Validate IGF-1 DES Use
Approved IGF-1 therapy does not validate IGF-1 DES use because mecasermin is full-length recombinant human IGF-1, supplied as a regulated medicine with defined labeling, dosing, warnings, manufacturing standards, and indications [13], 15. FDA labeling states that Increlex is for pediatric patients 2 years and older with severe primary IGF-1 deficiency or growth hormone gene deletion with neutralizing antibodies to GH [13].
IGF-1 DES lacks that approval framework. Evidence from approved mecasermin should be used as safety and context, not as permission to infer equivalent use.
Preclinical Research on IGF-1 DES
Preclinical research is where IGF-1 DES has its strongest evidence base. Studies in cells and animals help explain binding-protein biology, potency, growth-factor signaling, tissue growth, and glucose effects, but they cannot substitute for controlled human clinical trials.
Cell Culture Findings and Potency Questions
Cell culture findings helped establish why IGF-1 DES became scientifically interesting. Ballard and colleagues summarized that des(1-3)IGF-I was generally about 10-fold more potent than IGF-I in stimulating hypertrophy and proliferation of cultured cells, largely because of reduced IGF-binding protein interaction [1].
Another recombinant-analogue study found that changes affecting binding-protein interaction and receptor binding influenced biological potency [5]. These data support the “potent” descriptor in a laboratory sense, not a clinical claim that higher potency is safer or better.
Animal Models, Muscle Tissue, and Translational Limits
Animal models show that IGF-1 DES can influence growth-related endpoints under controlled experimental conditions. In rats after small-bowel resection, IGF-I and des(1-3)IGF-I were tested over a 7-day period using osmotic infusion pumps [7]. In renal insufficiency models, IGF-I and des(1-3)IGF-I were also studied for growth and nitrogen-balance effects [8].
The limitation is translation. Animal route, dose, disease model, age, tissue state, and monitoring do not match unsupervised human use.
Colostrum, Human Brain, and Tissue-Origin Research Context
Des(1-3)IGF-I has been reported in bovine colostrum, human brain, and porcine uterus, and it may result from post-translational cleavage of IGF-I [1]. This tissue-origin context explains why the peptide appears in discussions of natural IGF-1 processing.
It does not mean dietary colostrum products, synthetic peptides, or research chemicals produce the same biological exposure. Source, purity, formulation, route, and regulatory oversight all matter.
Safety, Side Effects, and Risk Profile
The safety profile of IGF-1 DES in humans is not well defined, so risk assessment must draw from IGF-1 biology, mecasermin labeling, animal data, and known growth-factor pathway concerns. The most important risks involve glucose lowering, tissue growth, abnormal proliferation, and unknown product quality.
Potential Side Effects Reported or Theoretically Expected
Potential side effects for IGF-1 DES are theoretical or extrapolated unless documented in direct human research. Mecasermin labeling lists common related adverse reactions in clinical trials, including hypoglycemia, local and systemic hypersensitivity, and tonsillar hypertrophy [13]. The label also includes warnings for intracranial hypertension, lymphoid tissue hypertrophy, slipped capital femoral epiphysis, scoliosis progression, malignant neoplasia, and benzyl alcohol risk in infants [13].
These are mecasermin label findings, not IGF-1 DES trial findings. They are still relevant because they show the seriousness of systemic IGF-1 pharmacology.
Hypoglycemia, Blood Sugar Level Changes, and Insulin-Like Effects
Hypoglycemia is a major concern for IGF-related therapy. FDA labeling states that severe hypoglycemia leading to hypoglycemic seizures has been observed with Increlex treatment and that IGF-1 has insulin-like hypoglycemic effects [13].
Animal studies add another caution: IGF-I variants that bind poorly to IGF-binding proteins produced more potent and prolonged hypoglycemic action than native IGF-I in pigs and marmoset monkeys [6]. For IGF-1 DES, glucose risk should not be minimized just because the peptide is often marketed in muscle-growth language.
Edema, Pain, Tissue Growth, and Unwanted Cell Proliferation
Edema, pain, injection-site reactions, local tissue changes, and unwanted growth effects are plausible concerns with growth-factor pathways. Mecasermin labeling includes injection-site rotation to reduce lipohypertrophy and warnings related to tissue growth, lymphoid hypertrophy, and malignancy [13].
IGF-1 receptor signaling also has a long-standing connection to cell proliferation and survival in cancer biology 17. That does not mean IGF-1 DES causes cancer in humans, but it does mean abnormal tissue growth and malignancy history deserve serious clinician-level caution.
Contraindications, Interactions, and Medical Supervision
Contraindications and interactions for IGF-1 DES are not defined in approved labeling because IGF-1 DES is not an approved drug. The safest educational approach is to identify risk categories from IGF-1 pharmacology and mecasermin labeling, then emphasize clinician-guided interpretation.
Diabetes, Insulin Resistance, and Glucose-Lowering Therapies
Diabetes, insulin resistance, fasting states, low carbohydrate intake, insulin use, sulfonylureas, and other glucose-lowering therapies are highly relevant because IGF-1 can lower blood sugar [13]. Mecasermin labeling recommends glucose monitoring during initiation and dose establishment and warns that treatment should be given around meals because of hypoglycemic risk [13].
For IGF-1 DES, there is no validated human monitoring protocol. That lack of protocol is itself a safety problem.
Cancer, Abnormal Tissue Growth, and IGF-1 Signaling Concerns
Cancer history and abnormal tissue growth require caution because IGF-1R signaling is involved in cellular proliferation, survival, and tumor biology [17]. FDA labeling contraindicates Increlex in pediatric patients with malignant neoplasia or a history of malignancy and warns about postmarketing reports of malignant neoplasms in pediatric patients receiving mecasermin [13].
No one should infer from this that IGF-1 DES has a quantified cancer risk in humans. The responsible conclusion is narrower: IGF pathway activation is not trivial in people with malignancy risk.
Pregnancy, Breastfeeding, Cardiovascular Disease, and Other Risk Groups
Pregnancy, breastfeeding, pediatric use, cardiovascular disease, kidney disease, liver disease, and endocrine disorders are special-population issues because growth-factor and glucose pathways interact with systemic physiology. FDA labeling for mecasermin states that safety and effectiveness are not established in children under 2 years of age and includes pregnancy and lactation sections in the approved label [13].
For IGF-1 DES, evidence gaps are larger. Anyone with these risk factors should treat the absence of reliable data as a reason for caution, not reassurance.
IGF-1 DES Dosage and Protocols in Context
IGF-1 DES dosage information should be framed as study context, not as a personal dosing recommendation. There is no FDA-approved IGF-1 DES dosage, and published IGF-1 DES dosing comes mainly from animal models rather than human therapeutic labeling.
What Dosage Has Been Used in Published Research?
Published preclinical studies provide some dose context. In a rat small-bowel resection model, des(1-3)IGF-I was administered at 0.96 mg/kg/day by osmotic infusion pump over 7 days [7]. In FDA-approved mecasermin labeling, the recommended starting dose for Increlex is 0.04 to 0.08 mg/kg twice daily, titrated up to 0.12 mg/kg twice daily if tolerated, but that dosing applies to mecasermin, not IGF-1 DES [13].
These numbers should not be merged into a personal IGF-1 DES protocol. Different molecule, different evidence base, different regulatory status.
Commonly Cited Protocol Ranges vs Evidence-Based Dosing
Commonly cited IGF-1 DES “protocol ranges” online are not the same as evidence-based dosing. Many online ranges come from bodybuilding forums, peptide sellers, or anecdotal reports rather than controlled human studies, so they should not be reproduced as medical dosing guidance.
Evidence-based dosing requires a defined drug product, indication, route, monitoring plan, population, adverse-event reporting, and clinical endpoint. IGF-1 DES does not currently have that package in approved human labeling.
Why IGF-1 DES Dosage Should Not Be Personalized From Online Protocols
IGF-1 DES dosage should not be personalized from online protocols because the most relevant safety issues include hypoglycemia, tissue-growth effects, drug interactions, and unknown product quality. Even mecasermin, an approved medicine, requires experienced physician supervision according to FDA labeling [13].
A dosing number without diagnosis, labs, indication, formulation, monitoring, and clinician oversight is not medical context. It is guesswork.
Reconstitution, Concentration, and Administration Routes
Reconstitution and administration information for IGF-1 DES should be understood as general educational context, not as instructions to prepare or inject a product. Reliable human administration guidance exists for approved mecasermin, while IGF-1 DES lacks approved route, frequency, and dosing instructions.
Reconstitution Concepts for Educational Dose Calculation
Reconstitution math is a concentration concept: amount of peptide divided by diluent volume equals concentration, and intended dose divided by concentration equals measured volume. This formula explains how concentration is calculated, but it does not establish whether a product is sterile, correctly labeled, clinically appropriate, or safe.
For approved mecasermin, reconstitution is not the relevant frame because Increlex is supplied as a ready solution at 10 mg/mL in FDA labeling [13]. IGF-1 DES products sold outside approved drug channels should not be assumed equivalent to approved medicines.
Subcutaneous and Intramuscular Administration in Literature Context
Approved mecasermin is administered subcutaneously, and FDA labeling states that Increlex should not be administered intravenously [13]. IGF-1 DES research has included experimental delivery methods such as osmotic infusion pumps in animal models [7].
Anti-doping research has also evaluated detection of IGF-I analogs, including des(1-3)-IGF-I, after intramuscular administration in a sports-testing context 20. That detection literature is not a therapeutic administration recommendation.
Route, Frequency, and Target Muscle Claims: What Remains Unclear
Route, frequency, and target muscle claims for IGF-1 DES remain unclear because reliable human dosing studies are lacking. Claims that local injection produces localized muscle growth are extrapolated from mechanistic ideas and animal research, not validated human protocols.
This is where evidence quality matters most. A plausible route does not equal a proven route, and a biological pathway does not equal a safe personal plan.
Regulatory Status and Legal Considerations
IGF-1 DES peptide is not an FDA-approved drug, while mecasermin is an approved recombinant human IGF-1 medicine for specific pediatric indications. Regulatory status changes how evidence, product quality, dosing, labeling, and safety claims should be interpreted.
Is IGF-1 DES Peptide FDA-Approved?
IGF-1 DES peptide is not listed in FDA labeling as an approved drug product for treatment of muscle growth, bodybuilding, recovery, anti-aging, sarcopenia, diabetes, injury, or any other therapeutic indication. The approved IGF-1 product discussed in this article is Increlex, which contains mecasermin and has a specific indication for pediatric severe primary IGF-1 deficiency or GH gene deletion with neutralizing antibodies to GH [13].
EMA also describes Increlex as a mecasermin solution for long-term treatment of patients aged 2 to 18 years with severe primary insulin-like-growth-factor-1 deficiency [14]. That European approval context still applies to mecasermin, not IGF-1 DES.
How IGF-1 DES Differs From Approved Mecasermin Therapy
Mecasermin is full-length recombinant human IGF-1, supplied under approved labeling with defined concentration, subcutaneous route, warnings, contraindications, and clinical-study data [13]. IGF-1 DES is a truncated IGF-1 variant with different binding-protein behavior and no comparable approved label [1].
This difference is not cosmetic. It affects pharmacology, safety assumptions, and legal interpretation.
Research Peptide Labeling, Compounding, and Quality Concerns
Research peptide labeling does not provide the same assurance as drug approval. Approved medicines are reviewed for manufacturing, labeling, safety, dosing, indication, and pharmacovigilance; unapproved peptides may lack those safeguards.
For IGF-1 DES, quality concerns are especially important because dose errors or contamination could intersect with hypoglycemia risk and growth-factor pathway effects. The article should not direct readers to vendors, sources, or purchasing options.
Evidence Limitations and Source Quality
The evidence for IGF-1 DES is limited mainly by the lack of controlled human clinical research, unclear long-term safety, and reliance on mechanistic extrapolation. Source quality is therefore central to interpreting every claim about benefits, dosage, side effects, and use.
Mechanistic Potency Does Not Equal Clinical Efficacy
Mechanistic potency does not equal clinical efficacy because a cell or animal model cannot reproduce human diagnosis, monitoring, comorbidities, duration, product quality, or adverse-event detection. IGF-1 DES may show stronger activity than native IGF-1 in certain models [1], but that does not prove a therapeutic outcome in people.
A useful rule: mechanism can explain why researchers care, but clinical evidence determines whether a treatment claim is justified.
How to Weigh PubMed, Clinical Trials, and Vendor Claims
Peer-reviewed PubMed studies, regulator labels, and clinical-trial registries should carry more weight than vendor pages, bodybuilding blogs, forums, or influencer content. FDA and EMA sources define what is approved for mecasermin [13], [14], while IGF-1 DES papers mainly define mechanism and preclinical context [1], [3], [7].
Vendor claims often blur these categories. A high-quality article should keep them separate.
Evidence Gaps in Long-Term Safety, Dosing, and Outcomes
Major IGF-1 DES evidence gaps include human pharmacokinetics, long-term safety, validated dosage, adverse-event rates, special-population risks, drug interactions, and clinical outcomes. These gaps matter more than the volume of online discussion.
When a peptide has strong online demand but weak human evidence, the safest interpretation is cautious, not promotional.
What Should Readers Discuss With a Clinician?
Readers should discuss IGF-1 DES questions with a qualified clinician by focusing on evidence quality, regulatory status, personal risk factors, and approved alternatives. The goal is not to obtain a peptide protocol; it is to understand whether a claim is medically credible.
Personal Risk Factors, Medications, and Blood Sugar Monitoring
Personal risk factors that matter include diabetes, hypoglycemia history, insulin use, glucose-lowering medications, cancer history, endocrine disorders, pregnancy, breastfeeding, cardiovascular disease, and pediatric growth concerns. IGF-1 therapies can affect glucose handling, and approved mecasermin labeling requires physician supervision and attention to hypoglycemia risk [13].
A practical clinician-discussion checklist:
- Current medications, especially insulin or glucose-lowering drugs
- Diabetes, insulin resistance, fasting hypoglycemia, or eating-pattern concerns
- Cancer history, abnormal growths, or unexplained tissue changes
- Pregnancy, breastfeeding, pediatric use, or fertility concerns
- Cardiovascular, kidney, liver, or endocrine conditions
- Whether any claim is supported by human evidence or only preclinical research
- Whether an approved alternative exists for the actual diagnosis
Questions About Approved Alternatives and Diagnostic Context
Approved alternatives depend on the medical problem being discussed. For severe primary IGF-1 deficiency, mecasermin is the regulated IGF-1 therapy with labeled pediatric indications [13], [14]. For muscle growth, bodybuilding, recovery, anti-aging, or target muscle claims, IGF-1 DES does not have approved therapeutic status.
The diagnostic context should come first. A peptide name should not come before a medical assessment.
Key Takeaways on Benefits, Risks, Dosage, and Research Quality
IGF-1 DES is best understood as an investigational IGF-1 variant with strong mechanistic interest and limited human therapeutic evidence. Its reduced IGF-binding protein interaction makes it biologically interesting, but also raises safety questions around potency, glucose effects, tissue growth, and systemic exposure.
The strongest conclusions come from approved labeling for mecasermin and peer-reviewed mechanistic or preclinical IGF-1 DES studies. Weaker claims, especially those about bodybuilding results, target muscle growth, or personal dosing protocols, should be treated cautiously and discussed with a qualified healthcare professional before any medical decision.
REFERENCES
- Ballard FJ, Wallace JC, Francis GL, Read LC, Tomas FM. Des(1–3)IGF-I: a truncated form of insulin-like growth factor-I. International Journal of Biochemistry & Cell Biology. 1996. PMID: 8930132. DOI: 10.1016/1357-2725(96)00056-8.
- Bailes J, Soloviev M. Insulin-Like Growth Factor-1 (IGF-1) and Its Monitoring in Medical Diagnostic and in Sports. Biomolecules. 2021. PMID: 33557137. DOI: 10.3390/biom11020217.
- Ross M, Francis GL. Insulin-like growth factor-binding proteins inhibit the biological activities of IGF-1 and IGF-2 but not des-(1-3)-IGF-1. Biochemical Journal. 1989. PMID: 2539101. DOI: 10.1042/bj2580267.
- Remacle-Bonnet M, et al. des-(1-3)-IGF-I, an insulin-like growth factor analog used to identify IGF-binding protein and receptor behavior. PubMed-indexed biomedical study. 1992. PMID: 1281142.
- Francis GL, Ross M, Ballard FJ, et al. Novel recombinant fusion protein analogues of insulin-like growth factor-I indicate the relative importance of IGF-binding protein and receptor binding for enhanced biological potency. Journal of Molecular Endocrinology. 1992. PMID: 1378742. DOI: 10.1677/jme.0.0080213.
- Tomas FM, Walton PE, Dunshea FR, Ballard FJ. IGF-I variants which bind poorly to IGF-binding proteins show more potent and prolonged hypoglycaemic action than native IGF-I in pigs and marmoset monkeys. Journal of Endocrinology. 1997. PMID: 9415072. DOI: 10.1677/joe.0.1550377.
- Lemmey AB, et al. IGF-I and the truncated analogue des-(1-3)IGF-I enhance growth in rats. PubMed-indexed animal study. 1991. PMID: 1996625.
- Martin AA, et al. IGF-I and its variant, des-(1-3)IGF-I, enhance growth in rats with renal insufficiency. PubMed-indexed animal study. 1991. PMID: 1928375.
- Gillespie C, et al. Enhanced potency of truncated insulin-like growth factor-I relative to IGF-I in lit/lit mice. PubMed-indexed animal study. 1990. PMID: 2280209.
- Yoshida T, Delafontaine P. Mechanisms of IGF-1-Mediated Regulation of Skeletal Muscle Hypertrophy and Atrophy. Cells. 2020. PMC: PMC7564605.
- LeRoith D, Holly JMP, Forbes BE. Insulin-like growth factors: ligands, binding proteins, and receptors. Molecular Metabolism. 2021. PMC: PMC8513159.
- De Meyts P. Insulin and IGF-I Receptor Structure and Binding Mechanism. NCBI Bookshelf. 2013.
- U.S. Food and Drug Administration. INCRELEX® (mecasermin) injection, for subcutaneous use: Prescribing Information. FDA label. Revised 2025.
- European Medicines Agency. Increlex: European Public Assessment Report overview. EMA. Current product overview.
- Australian Prescriber / NPS MedicineWise. Mecasermin for primary insulin-like growth factor-1 deficiency. Australian Prescriber. 2022. PMC: PMC9722352.
- Fintini D, et al. Profile of mecasermin for the long-term treatment of growth failure in children and adolescents with severe primary IGF-1 deficiency. Therapeutics and Clinical Risk Management. 2009. PMC: PMC2724186.
- Wang P, et al. Drugging IGF-1R in cancer: New insights and emerging opportunities. Cancer-related IGF-1 receptor review. 2022. PMC: PMC10066341.
- World Anti-Doping Agency. The Prohibited List. WADA official resource. Current anti-doping list resource.
- Adams GR. Localized infusion of IGF-I results in skeletal muscle hypertrophy in rats. Journal of Applied Physiology. 1998. PMID: 9572822.
- Mongongu C, et al. Detection of LongR3-IGF-I, Des(1-3)-IGF-I, and related IGF-I analogs in an anti-doping context. Drug Testing and Analysis. 2021. PMID: 33587816. :::
FAQs
What is IGF-DES peptide?
IGF-DES peptide is another way people refer to IGF-1 DES peptide, a shortened form of insulin-like growth factor 1 also described as des(1-3)IGF-I. It is discussed in research because it interacts differently with IGF-binding proteins than native IGF-1 [1]. IGF-DES is not the same as approved mecasermin therapy, and it should be interpreted as an investigational peptide rather than an approved treatment.
What is IGF-1 DES used for?
IGF-1 DES is mainly used in scientific discussion as a research peptide for studying IGF-1 signaling, growth-factor binding proteins, muscle-cell biology, tissue growth, and glucose-related effects. It is not FDA-approved for muscle growth, recovery, bodybuilding, anti-aging, or disease treatment [13]. Some uses discussed online are based on preclinical or mechanistic evidence, not strong human clinical studies.
What are the potential benefits of IGF-1 DES for muscle growth and recovery?
Potential benefits of IGF-1 DES for muscle growth and recovery remain mostly theoretical or preclinical. Laboratory and animal research suggests that IGF-1 DES may show stronger activity than native IGF-1 in some models because of reduced IGF-binding protein interaction [1], [3]. That does not prove human benefits for muscle mass, recovery, or performance, and bodybuilding claims should be treated as unsupported unless backed by clinical evidence.
What are the side effects or adverse effects of IGF-1 DES?
Side effects of IGF-1 DES are not well defined in human clinical studies. Safety concerns are inferred from IGF-1 biology, animal research, and mecasermin labeling, which includes risks such as hypoglycemia, hypersensitivity, tissue-growth effects, and malignancy-related warnings in specific contexts [13]. Possible adverse effects should be discussed with a licensed clinician, especially for people with diabetes, cancer history, or glucose-lowering medications.
What dosage and administration information exists for IGF-1 DES?
Dosage and administration information for IGF-1 DES is limited to study context, not approved human prescribing guidance. One rat study administered des(1-3)IGF-I at 0.96 mg/kg/day by osmotic infusion pump, while approved mecasermin dosing applies only to mecasermin, not IGF-1 DES [7], [13]. Any route of administration or dose discussion should be treated as educational, not a personal protocol.
How does IGF-1 DES compare to IGF-1 LR3?
IGF-1 DES and IGF-1 LR3 are both IGF-1 variants, but they are not interchangeable. IGF-1 DES is a truncated form missing the first three amino acids, while IGF-1 LR3 is a longer modified analogue designed differently [1], [5]. Comparisons should focus on structure, binding-protein interaction, evidence quality, safety uncertainty, and regulatory status rather than which peptide is “best” for muscle growth.
Contributing Authors
The following authors are recognized for published research that helped shape the scientific and clinical context discussed in this article.
F. John Ballard
Author profile: PubMed Author Search
F. John Ballard is recognized for published work on insulin-like growth factor biology, IGF-binding protein interactions, and des(1-3)IGF-I literature relevant to IGF-1 DES peptide pharmacology. His publications help frame why IGF-1 DES is discussed as a truncated insulin-like growth factor variant, how N-terminal structure affects binding-protein behavior, and why preclinical findings require careful interpretation before being applied to therapeutic claims. This work is especially relevant to the article’s discussion of peptide pharmacology, mechanism of action, and evidence limitations.
Selected publications:
- Des(1–3)IGF-I: a truncated form of insulin-like growth factor-I � International Journal of Biochemistry & Cell Biology, 1996. PMID: 8930132.
- A key functional role for the insulin-like growth factor 1 N-terminal pentapeptide � Biochemical Journal, 1989. PMID: 2730580.
Geoffrey L. Francis
Author profile: PubMed Author Search
Geoffrey L. Francis is recognized for peer-reviewed research on IGF analogues, receptor activity, and IGF-binding protein interactions. His published work is relevant to the article’s explanation of how IGF-1 DES differs from native IGF-1 and why altered binding-protein affinity can change biological activity in preclinical systems. These publications provide useful scientific background for distinguishing mechanism-focused peptide research from human clinical evidence, especially when interpreting claims about potency, bioavailability, and translational limitations.
Selected publications:
- Insulin-like growth factor-binding proteins inhibit the biological activities of IGF-1 and IGF-2 but not des-(1-3)-IGF-1 � Biochemical Journal, 1989. PMID: 2539101.
- Novel recombinant fusion protein analogues of insulin-like growth factor-I indicate the relative importance of IGF-binding protein and receptor binding for enhanced biological potency � Journal of Molecular Endocrinology, 1992. PMID: 1378742.
PUBLISHING FIELDS
- SEO Title: IGF-1 DES Peptide: Benefits, Dosage, Safety
- Meta Description: IGF-1 DES peptide guide covering uses, muscle-growth claims, side effects, dosage context, IGF-1 LR3 comparison, and research limits.
- Suggested URL Slug:
/igf-1-des-peptide - Page Type: Therapeutic Peptide Educational Article
- ArticleFormat: Therapeutic Peptide Educational Guide
- TargetPeptide: IGF-1 DES
- MainKeyword: igf-des peptide
- CanonicalKeyword: IGF-1 DES peptide
- ExactKeywordVariant: igf-des peptide
- AliasTerms: IGF-DES, des(1-3)IGF-I, des-(1-3)-IGF-I, IGF-1(4–70), truncated IGF-1, native IGF-1, IGF-1 LR3, mecasermin
- PeptideCategory: Investigational Peptide / Growth Factor Analog
- Primary Search Intent: Therapeutic informational
- Secondary Keywords: IGF-DES peptide, IGF-1 DES, des(1-3)IGF-I, IGF-1 LR3 vs IGF-1 DES, IGF-1 DES dosage, IGF-1 DES side effects, IGF-1 DES benefits, IGF-1 DES bodybuilding, IGF-1 DES muscle growth, IGF-1 DES mechanism, IGF-1 DES FDA approval, IGF-1 DES safety
- Evidence Levels Covered: approved context for mecasermin, clinical context for broader IGF-1 literature, limited human evidence, preclinical evidence, mechanistic evidence, unsupported online claims
- Excerpt: IGF-1 DES peptide is a truncated IGF-1 variant discussed for muscle growth, binding-protein interaction, and research use. This guide explains mechanism, benefits, dosage context, side effects, IGF-1 LR3 comparison, regulatory status, and evidence gaps.
- Suggested Tags: IGF-1 DES, IGF-DES, IGF-1 peptides, peptide research, growth factor analogs, peptide safety, dosage context, investigational peptides
- Featured Image Concept: Clinical evidence map showing IGF-1 DES peptide as an investigational growth factor analog compared with native IGF-1, IGF-1 LR3, and approved mecasermin context.
- Featured Image Alt Text: Scientific evidence map for IGF-1 DES peptide, native IGF-1, IGF-1 LR3, and approved mecasermin context.
- Suggested Schema: Article schema only.
INFOGRAPHIC BRIEFS
Infographic Brief 1
- Placement: After
## IGF-1 DES, Native IGF-1, and IGF-1 LR3 Explained - Title: IGF-1 DES vs Native IGF-1 vs IGF-1 LR3
- Purpose: Help readers understand why IGF-1 DES, native IGF-1, and IGF-1 LR3 should not be treated as interchangeable even though they are related to IGF-1 biology.
- Visual Format: Related peptide comparison chart.
- Key Labels: IGF-1 DES, native IGF-1, IGF-1 LR3, truncated form, binding proteins, receptor activity, evidence level, regulatory context
- Suggested Layout: Three side-by-side columns comparing structure, binding-protein interaction, evidence context, and regulatory interpretation. Use a small caution banner at the bottom: “Related compounds are not interchangeable.”
- Data or Concepts to Include: IGF-1 DES is missing the first three amino acids; native IGF-1 is the full-length 70-amino-acid growth factor; IGF-1 LR3 is a longer modified analogue; structural changes can affect binding-protein interaction, pharmacology, and evidence interpretation.
- Visual Style: Clean, clinical, editorial, lightly technical, with simple molecular icons and neutral comparison rows.
- Compliance Restrictions: No muscle transformation imagery, no bodybuilding imagery, no dosing visuals, no injection imagery, no “best peptide” language, no product vials, no vendor branding, no guaranteed outcome claims.
- Alt Text: Comparison chart showing how IGF-1 DES peptide differs from native IGF-1 and IGF-1 LR3.
- Full AI Image Prompt: Create a clean clinical editorial infographic titled “IGF-1 DES vs Native IGF-1 vs IGF-1 LR3.” Use three side-by-side comparison columns labeled “IGF-1 DES,” “Native IGF-1,” and “IGF-1 LR3.” Include rows for “Structure,” “Binding-protein interaction,” “Evidence context,” and “Regulatory interpretation.” Show IGF-1 DES as a truncated IGF-1 variant missing the first three amino acids, native IGF-1 as the full-length 70-amino-acid growth factor, and IGF-1 LR3 as a longer modified analogue. Add a bottom note: “Related compounds are not interchangeable.” Use a clean medical education style, neutral icons, soft grid lines, and no product, injection, bodybuilding, or sales imagery.
Infographic Brief 2
- Placement: After
## How Does IGF-1 DES Peptide Work? - Title: Proposed IGF-1 DES Mechanism
- Purpose: Explain the proposed mechanism of IGF-1 DES peptide through IGF-1 receptor signaling and reduced IGF-binding protein interaction.
- Visual Format: Mechanism of action diagram.
- Key Labels: IGF-1 DES, IGF-binding proteins, IGF-1 receptor, cell signaling, protein synthesis, tissue growth, glucose effects, safety uncertainty
- Suggested Layout: Left-to-right pathway: IGF-1 DES enters the research context, interacts less with binding proteins, reaches IGF-1 receptor signaling, then branches into studied pathways and safety concerns.
- Data or Concepts to Include: IGF-1 DES has reduced binding to IGF-binding proteins compared with native IGF-1; IGF-1 receptor signaling is tied to growth, metabolism, cell survival, and protein-synthesis pathways; reduced binding-protein interaction does not eliminate systemic risk.
- Visual Style: Scientific pathway diagram with abstract receptor and cell icons, restrained colors, and clear evidence caveats.
- Compliance Restrictions: No step-by-step use visuals, no injection tutorial imagery, no dosing, no reconstitution, no human transformation imagery, no claims of proven muscle growth, no vendor branding.
- Alt Text: Mechanism diagram showing IGF-1 DES peptide, IGF-binding proteins, IGF-1 receptor signaling, and safety uncertainty.
- Full AI Image Prompt: Create a clinical mechanism infographic titled “Proposed IGF-1 DES Mechanism.” Show a left-to-right flow diagram: “IGF-1 DES” leading to “Reduced IGF-binding protein interaction,” then to “IGF-1 receptor signaling.” From the receptor node, create three neutral branches labeled “cell signaling,” “protein-synthesis pathways,” and “glucose-related effects.” Add a separate caution branch labeled “systemic risk remains uncertain.” Use abstract molecules, receptor icons, and cell signaling arrows. Keep the visual educational and evidence-aware, with no injections, vials, bodybuilder imagery, dosing steps, or product branding.
Infographic Brief 3
- Placement: After
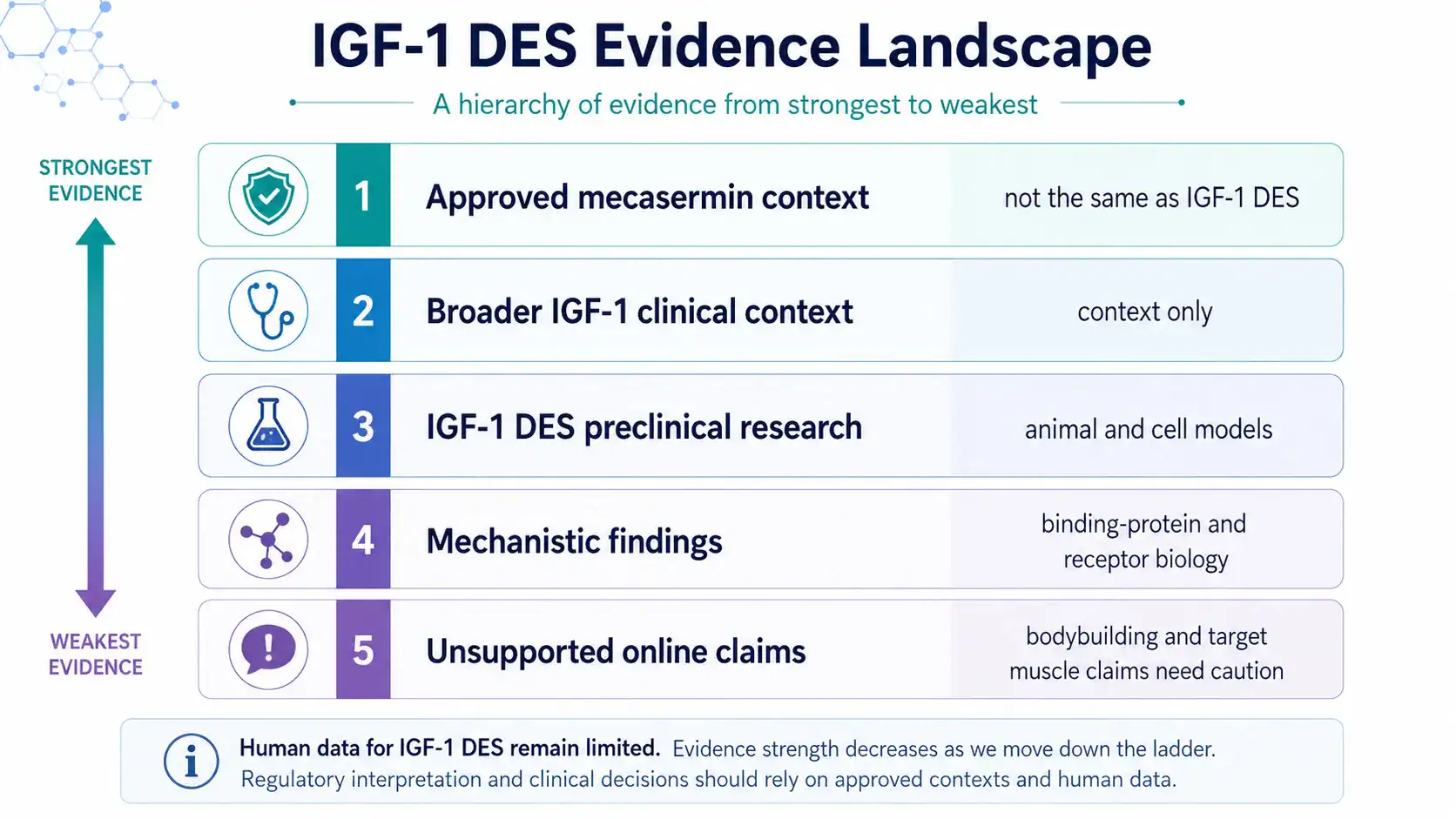
## Potential Benefits of IGF-1 DES Peptide - Title: IGF-1 DES Evidence Landscape
- Purpose: Summarize what the article says about benefit claims by evidence level so readers can separate mechanistic findings, preclinical findings, approved related-drug context, and unsupported claims.
- Visual Format: Evidence ladder.
- Key Labels: approved mecasermin context, broader IGF-1 evidence, IGF-1 DES preclinical research, mechanistic findings, online claims, evidence gaps, human data limited
- Suggested Layout: Vertical ladder from strongest to weakest evidence: approved mecasermin context, broader IGF-1 clinical context, IGF-1 DES preclinical research, mechanistic findings, unsupported online claims.
- Data or Concepts to Include: Mecasermin approval applies to specific pediatric indications, not IGF-1 DES; IGF-1 DES has preclinical and mechanistic evidence; bodybuilding, target muscle, and muscle-growth claims remain unsupported by strong human evidence.
- Visual Style: Editorial evidence hierarchy with clear labels, restrained icons, and a neutral medical palette.
- Compliance Restrictions: No before-and-after images, no muscle-gain imagery, no “proven benefits,” no result promises, no product sales imagery, no dosing or injection visuals.
- Alt Text: Evidence ladder for IGF-1 DES peptide showing approved related-drug context, preclinical research, mechanistic findings, and unsupported claims.
- Full AI Image Prompt: Create a clean medical evidence ladder infographic titled “IGF-1 DES Evidence Landscape.” Arrange five horizontal tiers from strongest to weakest evidence: “Approved mecasermin context,” “Broader IGF-1 clinical context,” “IGF-1 DES preclinical research,” “Mechanistic findings,” and “Unsupported online claims.” Add short notes beside each tier: “not the same as IGF-1 DES,” “context only,” “animal and cell models,” “binding-protein and receptor biology,” and “bodybuilding and target muscle claims need caution.” Use a clinical editorial design with no human transformation images, no bodybuilders, no product images, no injection visuals, and no guaranteed outcome language.
Infographic Brief 4
- Placement: After
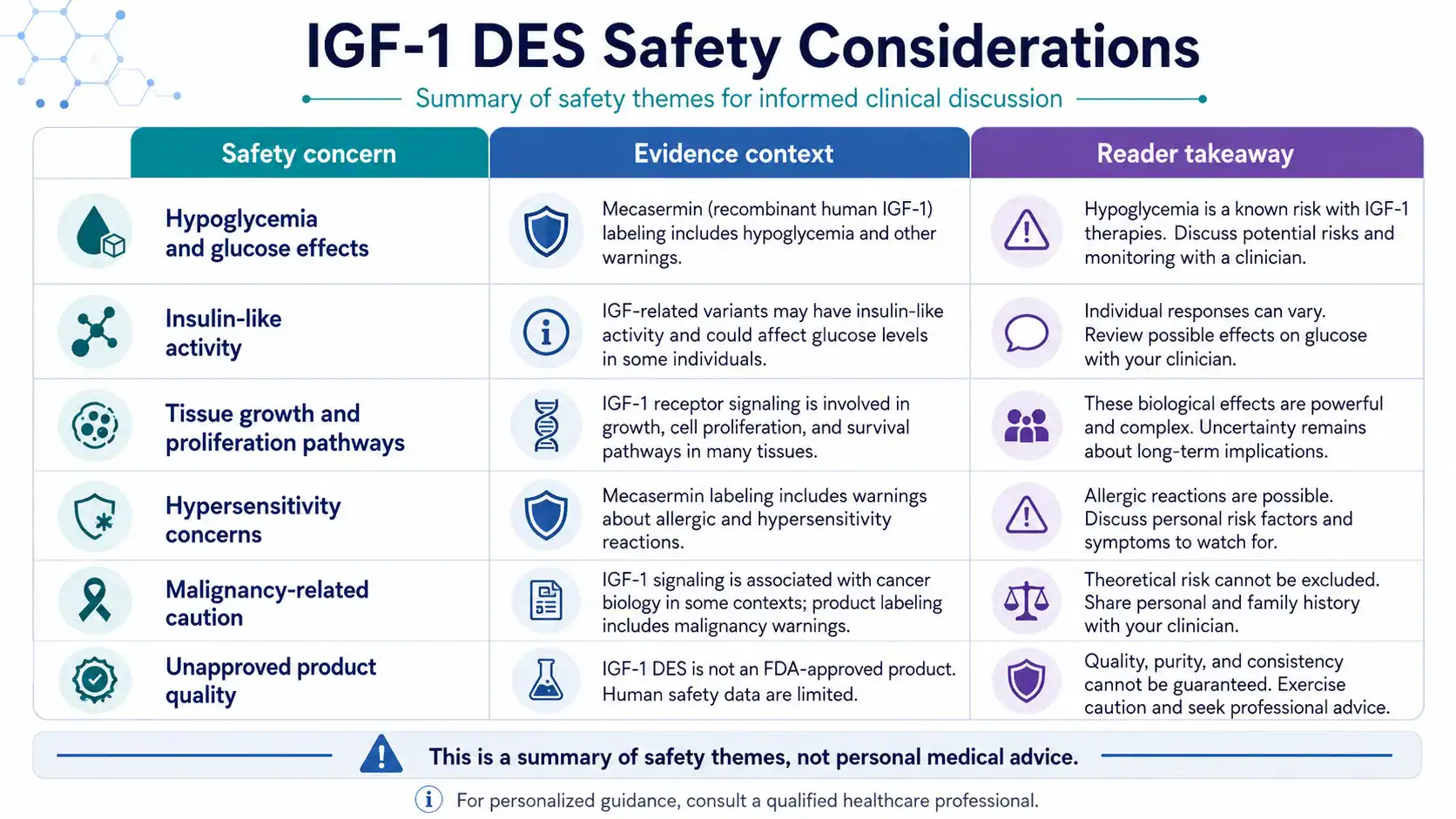
## Safety, Side Effects, and Risk Profile - Title: IGF-1 DES Safety Considerations
- Purpose: Give readers a quick visual summary of the safety themes already covered in the article, especially glucose effects, tissue-growth concerns, and uncertainty around unapproved peptide products.
- Visual Format: Side-effect and safety matrix.
- Key Labels: hypoglycemia, glucose, insulin-like effects, tissue growth, hypersensitivity, malignancy concerns, product quality, clinician discussion
- Suggested Layout: Matrix with rows for safety concern and columns for “Why it matters,” “Evidence context,” and “Reader takeaway.” Use caution icons without alarmist imagery.
- Data or Concepts to Include: Mecasermin labeling includes hypoglycemia and other warnings; IGF-related variants may have glucose-related effects; IGF-1 receptor signaling is tied to cell growth and proliferation pathways; IGF-1 DES human safety data are limited.
- Visual Style: Clinical safety matrix, clear, calm, and non-alarmist.
- Compliance Restrictions: No emergency-room imagery, no syringes, no injection sites, no fear-based cancer imagery, no dosage directions, no product packaging, no unsafe self-use framing.
- Alt Text: Safety matrix for IGF-1 DES peptide covering hypoglycemia, glucose effects, tissue growth, and product-quality concerns.
- Full AI Image Prompt: Create a clinical safety matrix infographic titled “IGF-1 DES Safety Considerations.” Use a three-column table labeled “Safety concern,” “Evidence context,” and “Reader takeaway.” Include rows for “hypoglycemia and glucose effects,” “insulin-like activity,” “tissue growth and proliferation pathways,” “hypersensitivity concerns,” “malignancy-related caution,” and “unapproved product quality.” Use calm caution icons, neutral colors, and concise labels. Do not include syringes, injection sites, product vials, hospital emergency imagery, fear-based cancer visuals, dosing directions, or sales imagery.
Infographic Brief 5
- Placement: After
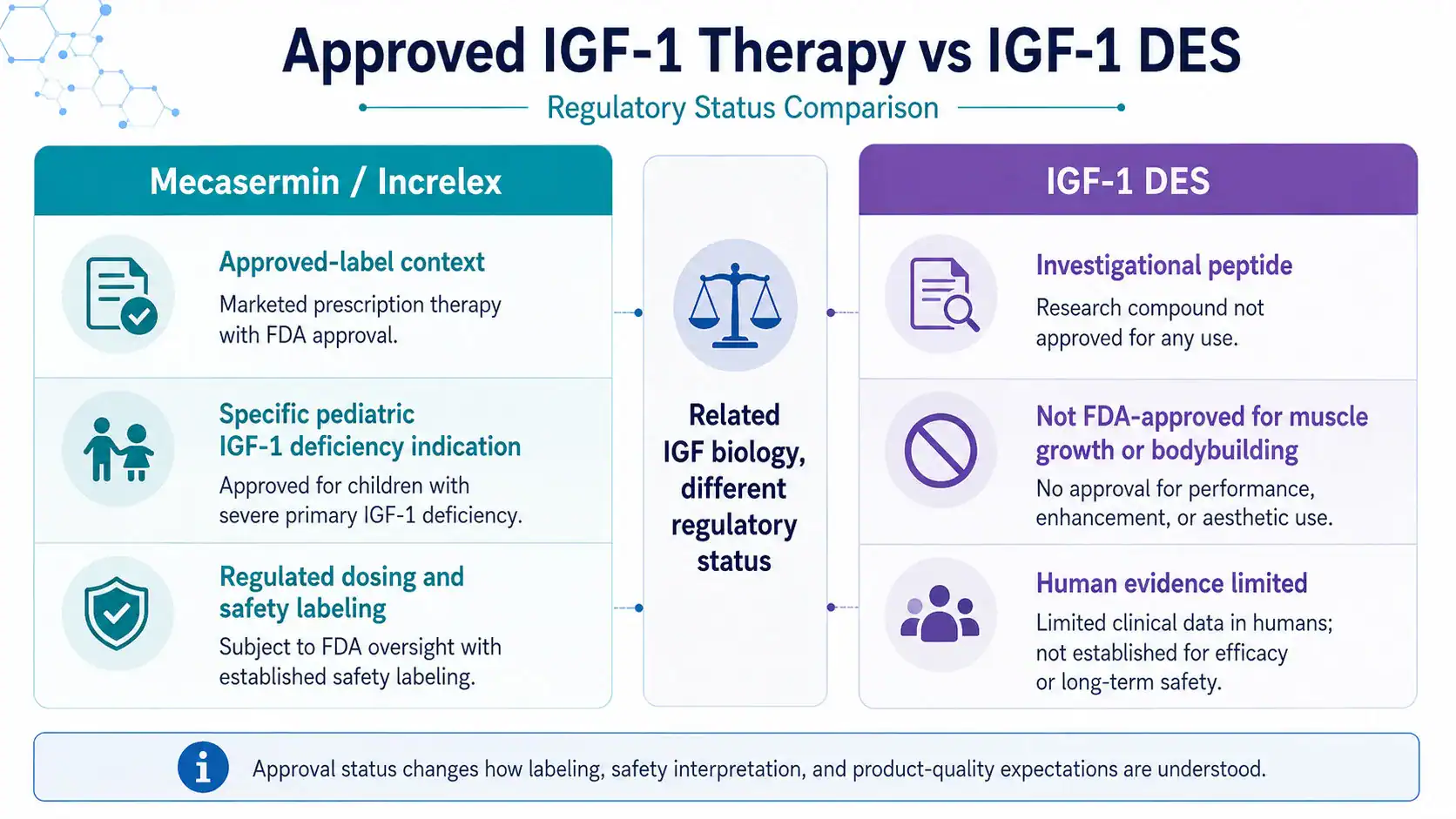
## Regulatory Status and Legal Considerations - Title: Approved IGF-1 Therapy vs IGF-1 DES
- Purpose: Clarify that approved mecasermin therapy and IGF-1 DES peptide are not the same regulatory category.
- Visual Format: Approved vs investigational status map.
- Key Labels: IGF-1 DES, mecasermin, Increlex, FDA-approved context, EMA context, investigational peptide, unapproved peptide, labeling matters
- Suggested Layout: Two-lane status map. Left lane: mecasermin / Increlex with approved-label context. Right lane: IGF-1 DES with investigational and unapproved status. Center divider: “Related IGF biology, different regulatory status.”
- Data or Concepts to Include: Mecasermin is approved for specific pediatric severe primary IGF-1 deficiency context; IGF-1 DES is not FDA-approved for muscle growth, recovery, bodybuilding, anti-aging, or disease treatment; approval status affects dosing, safety, labeling, and product-quality interpretation.
- Visual Style: Clean regulatory map with document icons, clear lane labels, and no promotional design elements.
- Compliance Restrictions: No purchase cues, no vendor or pharmacy imagery, no product bottles, no “legal to use” claims, no self-treatment framing, no dosing instructions, no injection imagery.
- Alt Text: Regulatory status map comparing approved mecasermin context with investigational IGF-1 DES peptide.
- Full AI Image Prompt: Create a clean regulatory status infographic titled “Approved IGF-1 Therapy vs IGF-1 DES.” Use a two-lane map. The left lane is labeled “Mecasermin / Increlex” and includes “approved-label context,” “specific pediatric IGF-1 deficiency indication,” and “regulated dosing and safety labeling.” The right lane is labeled “IGF-1 DES” and includes “investigational peptide,” “not FDA-approved for muscle growth or bodybuilding,” and “human evidence limited.” Add a center divider reading “Related IGF biology, different regulatory status.” Use document icons, neutral medical styling, and no product packaging, vendor branding, injection imagery, dosing instructions, or sales cues.