PE-22-28 Peptide: Benefits, Uses, Side Effects, Dosage, and Research
PE-22-28 peptide is an investigational, spadin-related research peptide discussed in connection with sortilin-derived peptide biology and TREK-1 potassium channel literature 1 2. This educational article separates approved medical use, clinical evidence, preclinical research, safety questions, dosage information, administration-route context, and unsupported online claims. It does not provide personal medical advice, dosing instructions, self-administration guidance, or purchasing recommendations.
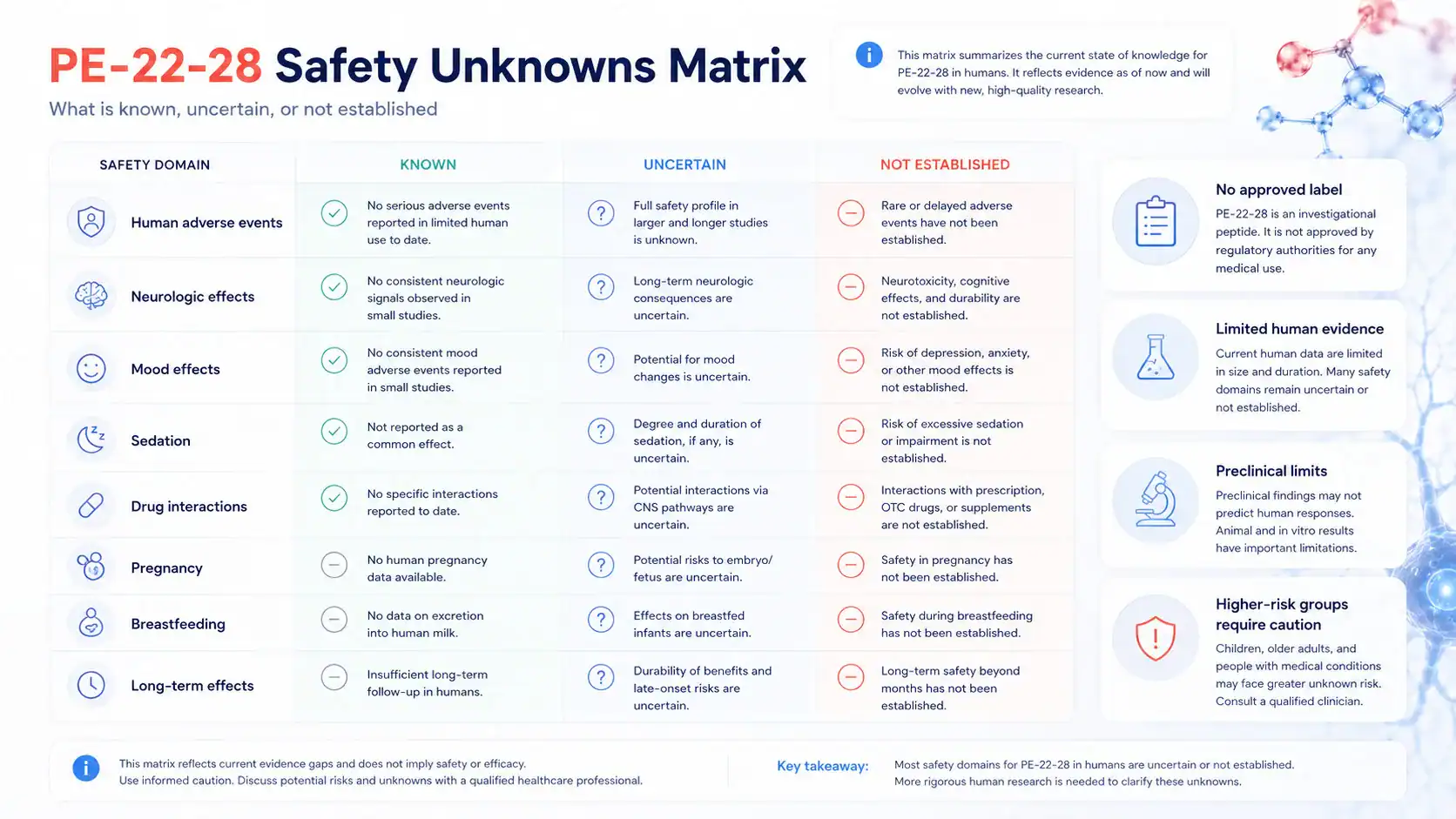
- PE-22-28 is best described as a research-stage, spadin-related peptide fragment discussed in the same scientific lane as sortilin-derived spadin and TREK-1 channel modulation [1] [2].
- TREK-1 is a two-pore-domain potassium channel encoded by KCNK2, and it is involved in neuronal excitability and potassium conductance 6 7.
- No approved therapeutic use for PE-22-28 was identified in major FDA or EMA medicine databases under this name, so it should not be treated as an approved medication 4 5.
- Human clinical evidence appears absent or very limited under the exact PE-22-28 name; ClinicalTrials.gov search results should be checked directly when evaluating trial status 3.
- Potential benefits such as mood-related, antidepressant-like, neurogenesis, memory, or neuroprotective claims are mainly preclinical or mechanistic unless supported by human studies [1] 9 18.
- Side effects, contraindications, interactions, and long-term effects are not well characterized in humans for PE-22-28, because there is no mature approved-label or clinical-trial safety database under this name [3] [4].
- Dosage information should be limited to approved labels or published study protocols; because PE-22-28 has no approved label, animal-study dosing should not be converted into personal dosing advice [4] 16.
Fast Answer
PE-22-28 peptide is an investigational spadin-related peptide fragment discussed for TREK-1 potassium channel research, mood biology, and neuroplasticity hypotheses [1] [2]. People search for it because of online claims about mood, memory, and brain support, but the public evidence base appears mainly preclinical, not established clinical therapy [2] [3]. No FDA- or EMA-approved PE-22-28 indication or approved dosage was identified under this name [4] [5]. Safety, interactions, and long-term human effects remain uncertain.
What Is the PE-22-28 Peptide?
PE-22-28 is generally discussed as a synthetic research peptide related to the spadin/sortilin-derived peptide research program. Spadin itself was described as a peptide derived from the sortilin propeptide and studied as a TREK-1 blocker with antidepressant-like effects in rodent models [1].
The key safety point is that PE-22-28 is not the same as an approved peptide drug with regulator-reviewed labeling, manufacturing controls, approved indications, and approved dosing. FDA and EMA medicine databases should be used to verify approval status for any claimed therapeutic peptide product [4] [5].
How Do PE-22-28, PE 22-28, and Sortilin-Derived Names Relate?
The terms PE-22-28, PE 22-28, and PE(22–28) are naming variants that usually point to a shortened peptide fragment or analog discussed in the broader spadin literature. Spadin is commonly described as a sortilin-derived peptide, and the PE numbering refers to positions in the propeptide-derived research nomenclature rather than to a marketed medication name [1] [2].
This naming difference matters for evidence review. Searching only one spelling can miss related literature, while broad searches may also capture spadin, sortilin, KCNK2, and TREK-1 papers that are relevant mechanistically but not necessarily direct human evidence for PE-22-28 [2].
Spadin is the best-described parent structure in this research area. It was reported to block rodent TREK-1 channels and produce antidepressant-like behavioral effects in animal studies [1].
PE-22-28 is discussed as a shortened analog or peptide fragment in that same research lane, but direct clinical conclusions about PE-22-28 should not be imported from spadin without caution. TREK-1 is an ion channel, not a conventional “TREK-1 receptor,” and it is encoded by the KCNK2 gene [6] [7].
Fast Evidence Snapshot for PE-22-28
The evidence landscape for PE-22-28 is uneven. The strongest public evidence is not an approved-label or large human-trial evidence base; it is the mechanistic and preclinical literature around spadin, TREK-1, KCNK2, rodent mood models, and potassium-channel pharmacology [1] [6] 8.
| Evidence Area |
What Has Been Studied |
Evidence Level |
What It Can and Cannot Show |
| Regulatory status |
FDA and EMA medicine databases do not show an approved PE-22-28 product under this name [4] [5] |
Approved-use evidence absent |
Supports regulatory caution; does not prove safety or lack of biological activity |
| Human trials |
ClinicalTrials.gov search under PE-22-28 should be checked for registered trials [3] |
Clinical evidence absent or not readily identified |
Cannot establish clinical efficacy, optimal dose, or human safety profile |
| TREK-1 mechanism |
TREK-1/KCNK2 potassium-channel biology and spadin blockade have been studied [1] [6] [8] |
Mechanistic / preclinical |
Supports biological plausibility, not approved therapeutic use |
| Mood-related models |
TREK-1 knockout and spadin studies reported antidepressant-like effects in rodents [1] [9] |
Preclinical |
Can guide hypotheses; cannot prove treatment effects in major depressive disorder |
| Neurogenesis claims |
Spadin literature and antidepressant research discuss hippocampal neurogenesis pathways [1] [18] |
Preclinical / mechanistic |
Suggests a possible pathway; does not confirm human cognitive or mood benefit |
| Dosage and safety |
No approved PE-22-28 label was identified; animal protocols are not personal dosing advice [4] [16] |
Evidence-limited |
Supports caution in interpreting online dosage claims |
What Is Known About Approval, Clinical Evidence, and Preclinical Status?
The public evidence base supports three practical distinctions. PE-22-28 is not identified as an FDA- or EMA-approved medicine under this name, it does not appear to have a clear registered clinical-trial footprint under the exact PE-22-28 search term, and its scientific rationale mainly comes from spadin/TREK-1 preclinical research [1] [3] [4] [5].
That distinction is important because approved drugs, investigational compounds, and research peptides are evaluated differently. FDA clinical research guidance explains that clinical trials are the process used to evaluate whether a drug is safe and effective in humans for a defined use [16].
Key Takeaways for Therapeutic Decision-Making
Therapeutic claims about PE-22-28 should be graded by evidence level. Approved labeling would be strongest, human clinical trials would be next, animal and cell research would be hypothesis-generating, and online anecdotes would be the weakest form of evidence [16].
For readers, the safest interpretation is that PE-22-28 remains a research-stage peptide. Any medical decision involving mood disorders, psychiatric medication, neurologic disease, pregnancy, breastfeeding, or seizure history should be discussed with a licensed clinician rather than guided by online claims.
How Does PE-22-28 Work?
PE-22-28 is thought to belong to the same mechanistic family as spadin, which was studied as a blocker of the TREK-1 potassium channel [1]. The proposed mechanism of action centers on potassium-channel modulation, neuronal excitability, and downstream effects on neurotransmission and neuroplasticity, but direct human pharmacodynamics for PE-22-28 are not established [2] [3].
Proposed Mechanism of Action at TREK-1
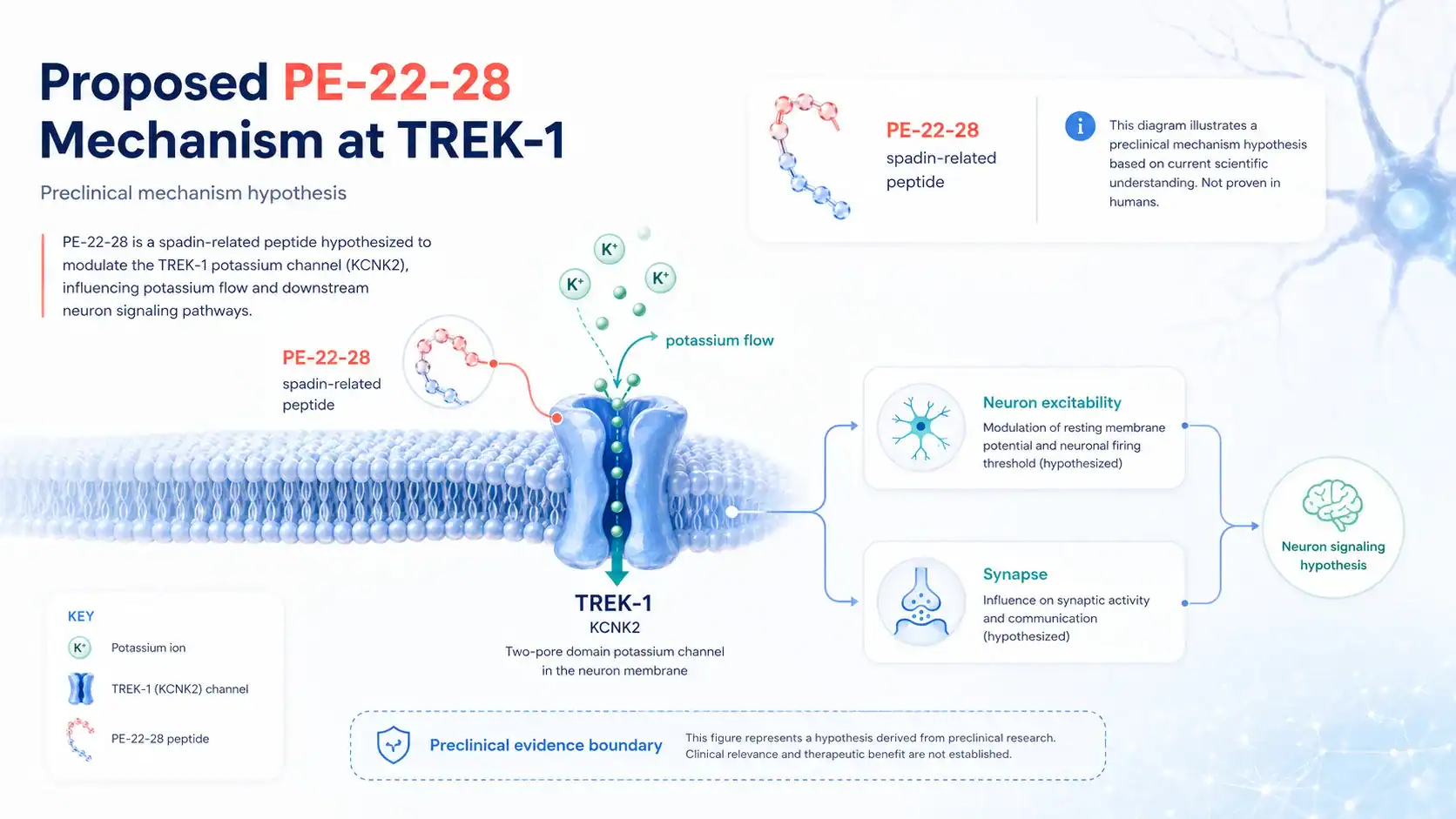
TREK-1 is a two-pore-domain potassium channel that contributes to background potassium currents, which help shape the resting membrane potential and excitability of neurons [8]. Spadin was reported to inhibit TREK-1 activity in preclinical experiments, and this led researchers to explore TREK-1 blockers as possible antidepressant drug candidates [1].
For PE-22-28, the proposed mechanism is usually discussed by analogy to spadin and shortened analogs of spadin. That analogy is useful for hypothesis-building, but it is not enough to establish human therapeutic effects, binding selectivity, bioavailability, or safety.
How Might Potassium Channel Inhibition Affect Neuron Signaling?
Potassium channels influence how easily a neuron fires an action potential. When background potassium conductance changes, neuron excitability and synaptic signal patterns may also change, depending on the channel, cell type, brain region, and dose [8].
In mood research, TREK-1 is interesting because TREK-1 knockout mice showed depression-resistant behavioral phenotypes in a landmark preclinical study [9]. However, a mouse model cannot fully reproduce major depressive disorder, and potassium channel inhibition in the nervous system may have effects beyond mood regulation [8] [9].
Why Mechanism Does Not Prove Clinical Benefit
A mechanism can make a peptide biologically plausible without proving that it helps patients. Clinical trials are needed because animal behavior, receptor or ion-channel pharmacology, and in vitro findings may not translate into human efficacy or safety [16].
This distinction is especially important for PE-22-28 therapy claims. A claim that PE-22-28 binds or modulates a channel does not automatically establish an antidepressant effect, memory benefit, neuroprotective effect, or safe human dose.
TREK-1, Spadin, and Mood Regulation
TREK-1 has become a recurring target in mood-disorder research because genetic and pharmacologic studies connect this potassium channel to stress-related and depression-like behavior in model organisms [1] [9]. PE-22-28 is part of that discussion because of its relationship to the spadin research family.
What Is the TREK-1 Potassium Channel?
TREK-1 is a two-pore-domain potassium channel encoded by KCNK2 [6]. UniProt identifies human KCNK2/TREK-1 as a potassium channel protein, and broader ion-channel reviews describe K2P channels as background channels that influence membrane potential and cellular excitability [7] [8].
Calling TREK-1 a “TREK-1 receptor” is imprecise. In pharmacology, the more accurate term is TREK-1 channel or TREK-1 potassium channel [6] [7].
How Might Analogs of Spadin Affect Neurotransmission?
Spadin was reported to affect serotonergic neurotransmission and produce antidepressant-like effects in preclinical models [1]. This is one reason PE-22-28 and other analogs of spadin are discussed in the context of mood regulation.
Still, neurotransmission is complex. Serotonin, dopamine, synaptic plasticity, prefrontal cortex circuits, hippocampal pathways, and raphe nuclei activity all interact in depression biology, and a single peptide mechanism cannot be assumed to reproduce the effects of approved antidepressant drugs 11 12.
Potential Benefits of PE-22-28 Peptide
The potential benefits of PE-22-28 peptide should be framed as research hypotheses, not established medical outcomes. The most common claims involve antidepressant-like activity, neurogenesis, mood-enhancing effects, cognition, memory, and brain support, but direct human evidence appears limited under the PE-22-28 name [2] [3].
What Research Suggests About Antidepressant-Like Effects
The most relevant evidence comes from the spadin and TREK-1 literature. Spadin was reported to produce antidepressant-like effects in animal studies, and TREK-1 knockout mice showed reduced depression-like behavior in preclinical experiments [1] [9].
This does not mean PE-22-28 is proven to treat major depressive disorder. Major depressive disorder is a clinical diagnosis, and treatment decisions are typically based on clinical assessment, psychotherapy options, approved medications, patient risk factors, and guideline-supported care [11].
Can PE-22-28 Induce Neurogenesis in the Hippocampus?
Spadin research reported effects related to neurogenesis, and broader antidepressant research has studied neurogenesis in the hippocampus as one possible contributor to behavioral effects in rodents [1] [18]. This creates a plausible reason for interest in PE-22-28 and related peptide fragments.
The evidence should stay in its lane. A finding that a compound may induce neurogenesis in a mouse model does not prove improved memory, resilience, or mood in humans.
Memory, Cognition, and Brain Support Claims
Memory and cognition claims are common in online discussions of neuroactive peptides, but PE-22-28 has not been established as a cognitive-enhancement medication. Searches of PubMed and ClinicalTrials.gov under PE-22-28 do not provide the kind of large human evidence base that would be needed to support strong brain-support claims [2] [3].
The term “brain support” is also broad. It can refer to neuroprotection, synaptic plasticity, neurotrophic factor signaling, mood regulation, fatigue, or mental clarity, and each claim needs separate evidence rather than a single umbrella promise [8] 10.
What Is PE-22-28 Used For or Studied For?
PE-22-28 is best discussed as a research peptide studied or proposed in relation to TREK-1 biology, spadin analog development, and mood-related preclinical work. It should not be described as an approved treatment for depression, anxiety, stroke, post-stroke depression, memory impairment, or any other condition unless regulator-approved labeling or human clinical evidence supports that claim [3] [4] [5].
How Do Researchers Model Mood Disorders and Behavioral Despair?
Preclinical mood research often uses rodent tests such as the forced swim test to screen antidepressant-like activity 17. These models can detect behavioral effects, but they are not the same as diagnosing or treating major depressive disorder in a patient.
That limitation matters for PE-22-28. Effects in rodents can help researchers decide whether a pathway deserves further study, but they cannot establish human efficacy, dose, safety, or patient outcomes.
Post-Stroke Depression, Anxiety, and Neuroprotective Hypotheses
Post-stroke depression is a recognized clinical problem, and professional scientific statements describe it as common and clinically important after stroke 20. TREK-1 has also been studied in neuroprotection and ischemia-related biology, which may explain why some researchers connect TREK-1 blockers, spadin analogs, and post-stroke mood hypotheses [10].
Even so, PE-22-28 is not established as a post-stroke depression therapy. Claims about anxiety, neuroprotective effects, protective effects, or mood-enhancing effects should be treated as preclinical, mechanistic, or unsupported unless human trials are available [2] [3].
Research on PE-22-28: What Studies Have Found
Research on PE-22-28 should be read with a source-quality filter. The closer a source is to peer-reviewed spadin/TREK-1 science, official trial registries, or regulator databases, the more useful it is for medical interpretation; vendor pages and anecdotal reports are not adequate evidence for therapeutic claims.
What Have Mouse and Rodent Animal Models Reported?
The strongest related animal evidence comes from TREK-1 and spadin studies. TREK-1 knockout mice showed depression-resistant phenotypes, and spadin was reported to produce antidepressant-like effects in mice while acting as a TREK-1 blocker [1] [9].
These findings are important but limited. Mouse behavior tests are designed for research screening, not for proving human antidepressant activity, and the term “antidepressant-like effects in animal studies” is more accurate than “antidepressant effects” when discussing PE-22-28 [17].
In Vitro and Mechanistic Research Findings
In vitro and electrophysiology research can examine whether a compound changes TREK-1 channel activity, receptor-binding behavior, or ion-channel function. Spadin’s TREK-1 activity was studied in this mechanistic way, and K2P channel reviews help explain why these background potassium channels matter for neuron signaling [1] [8].
For PE-22-28, in vitro findings would still need to be connected to pharmacokinetics, bioavailability, tissue distribution, dose-response, and safety. A potent channel effect in a lab setting does not prove therapeutic effects in humans.
Evidence Grading: Strong, Preliminary, or Unsupported Claims
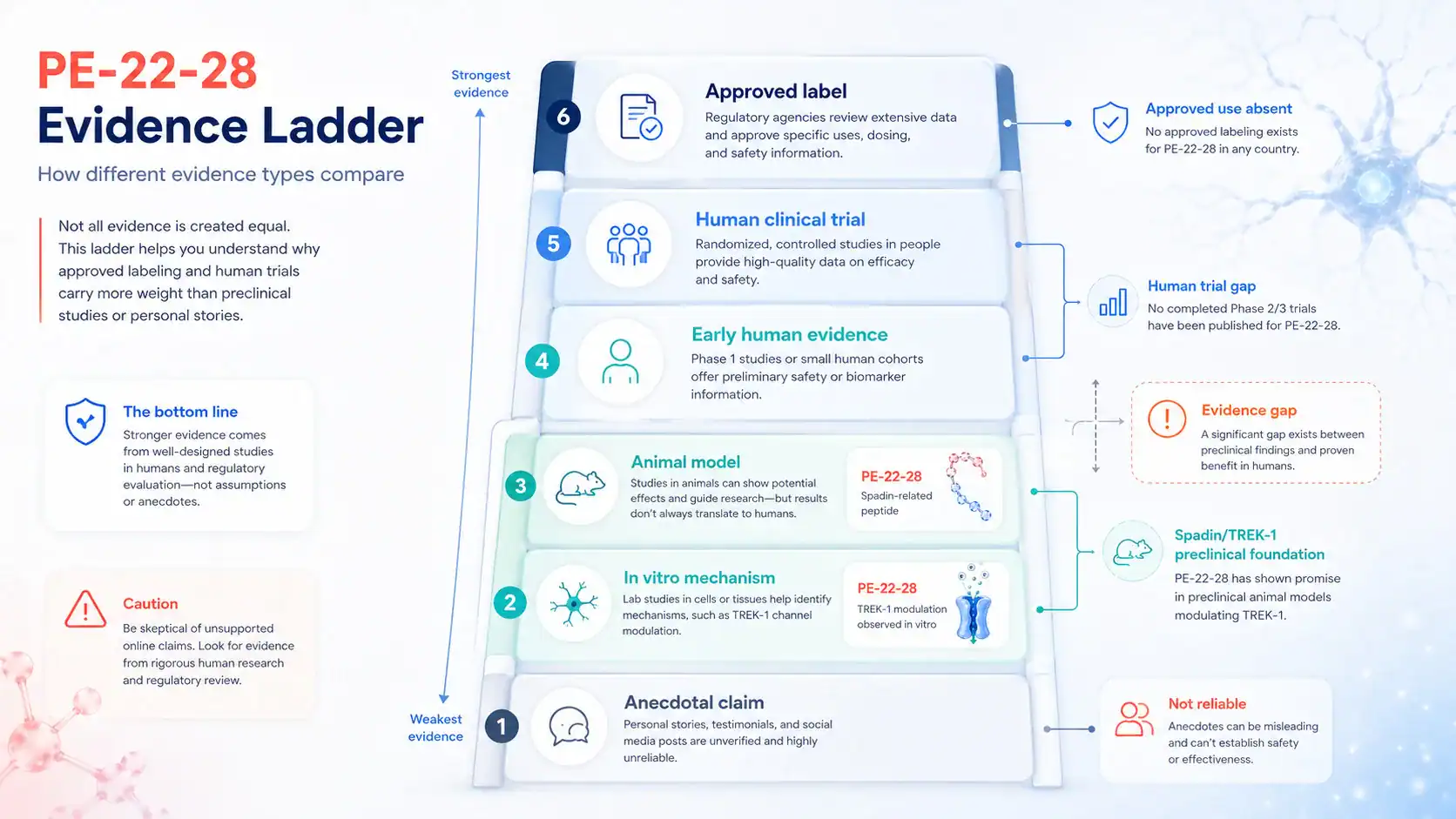
A practical evidence ladder for PE-22-28 looks like this: approved labeling is strongest, registered and published human trials come next, animal studies are preclinical, cell studies are mechanistic, and anecdotes are unsupported. FDA clinical research materials describe why human trials are needed before a drug’s safety and effectiveness can be established for patients [16].
Using that ladder, most PE-22-28 claims fall into the preclinical, mechanistic, or unsupported categories. Claims about guaranteed mood improvement, memory enhancement, or safe long-term peptide therapy are not supported by the evidence level currently visible in major public databases [2] [3] [4].
What Does Human Evidence Show About PE-22-28?
Human evidence is the biggest gap for PE-22-28. Without well-designed human studies, it is not possible to determine whether preclinical findings translate to patients, whether adverse events emerge with repeated exposure, or whether any benefit outweighs risk.
Are There Published Human Studies?
A ClinicalTrials.gov search under PE-22-28 does not identify a clear registered clinical-trial evidence base under that exact term at the time of writing [3]. PubMed searches under PE-22-28, spadin, and TREK-1 should also be checked, but the indexed literature appears far stronger for spadin/TREK-1 mechanisms than for PE-22-28 human outcomes [2].
This does not prove PE-22-28 has no biological activity. It means the public clinical evidence base is not strong enough to support treatment claims, dosage recommendations, or general safety conclusions.
Why Preclinical Development Limits Therapeutic Claims
Preclinical development is useful because it can identify mechanisms, target engagement, and early safety concerns. It is limited because animals and cell systems cannot fully predict human pharmacology, psychiatric outcomes, drug interactions, or rare adverse events [16].
For PE-22-28, the responsible conclusion is cautious. The peptide may be scientifically interesting, but it should not be positioned as an established treatment for a mood disorder, cognitive problem, stroke-related condition, or neurologic disease without human evidence and regulatory review.
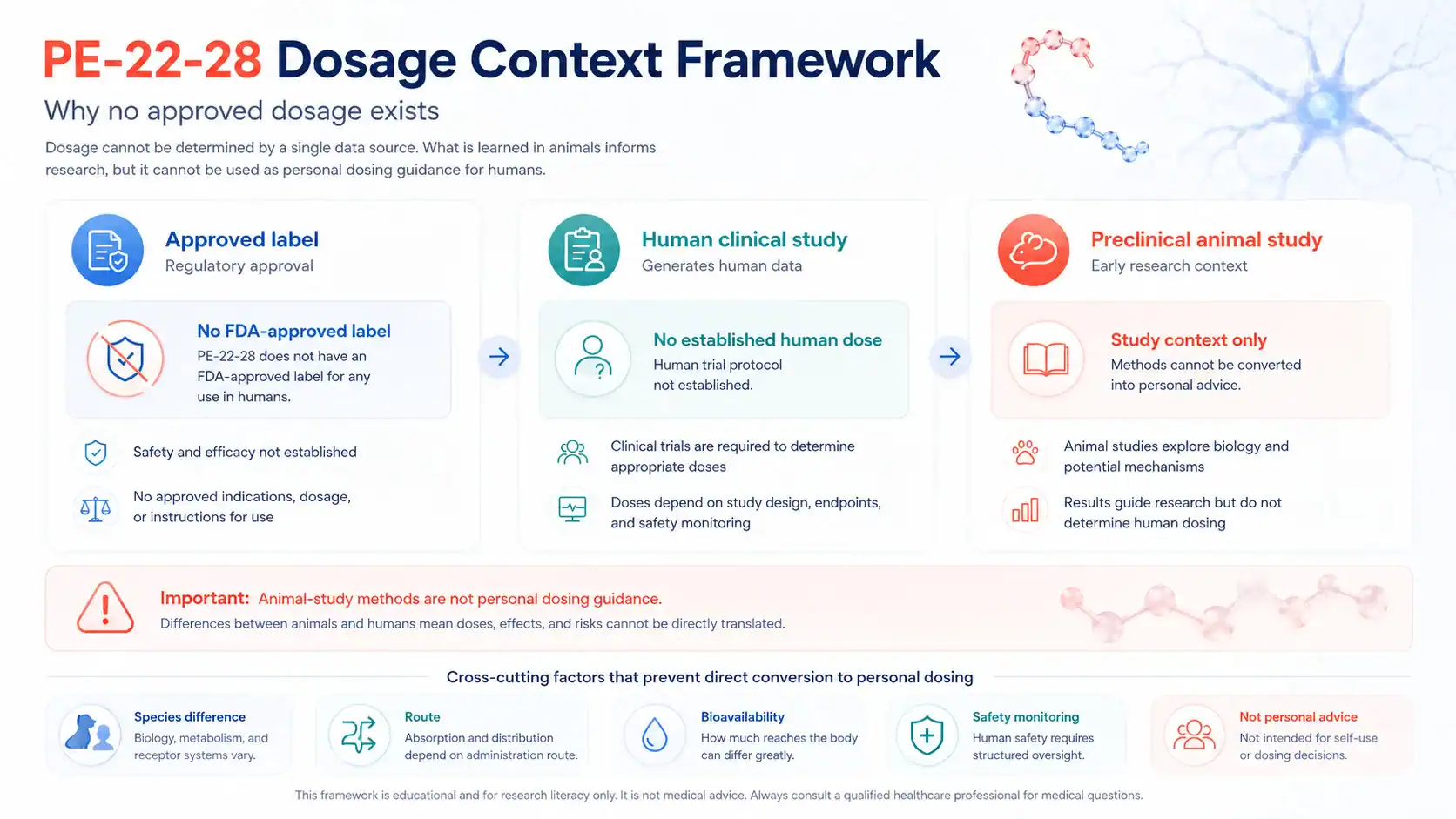
There is no approved PE-22-28 dosage in FDA or EMA labeling under this name, because no approved PE-22-28 medicine was identified in those medicine databases [4] [5]. Any dosage information discussed online should therefore be separated from approved-label dosing, clinical-trial dosing, and animal-study methods.
Is There an Approved PE-22-28 Dosage?
No FDA-approved prescribing information for PE-22-28 was identified under this name in Drugs@FDA, and no EMA-approved medicine listing was identified under this name in the EMA medicines database [4] [5]. That means there is no regulator-reviewed approved dosage, labeled indication, contraindication list, adverse-reaction table, or administration instruction for PE-22-28 as a medicine.
This is a major difference between PE-22-28 and approved drugs. Approved labels are evaluated for a specific product, population, indication, route, dose, and risk profile; PE-22-28 does not have that type of public approved-label framework [4] [16].
What Doses Have Been Reported in Preclinical Research?
Published spadin-related animal studies include experimental dosing methods, but those methods are designed for controlled research in model organisms [1]. They should not be converted into human dosing, beginner dosing, cycles, stacks, or self-treatment protocols.
For PE-22-28 specifically, the practical dosing conclusion is that no approved-label or established human clinical-trial dose is available from major public regulatory databases under this name [3] [4] [5]. Study doses should not be interpreted as personal dosing advice.
Why Animal Doses Are Not Personal Dosing Advice
Animal doses differ from human medical dosing because species, metabolism, route, formulation, endpoint, exposure, and safety monitoring differ. FDA clinical research guidance emphasizes that human studies are a separate step in evaluating drugs for safety and effectiveness [16].
This is why a mouse dose from an animal model cannot be translated into a patient protocol. It also explains why claims about “best PE-22-28 dosage” or “PE-22-28 protocol” should be viewed as high-risk if they are not grounded in approved labeling or clinician-supervised clinical research.
What Administration Routes Are Discussed in the Literature?
Administration route affects bioavailability, brain exposure, duration of action, safety monitoring, and interpretation of study findings. For PE-22-28, public therapeutic discussion should stay at the level of literature context and should not become injection, mixing, reconstitution, or self-administration instruction.
Which Routes Are Used in Research Settings?
Spadin-related studies used controlled experimental administration methods in animal research settings, but those methods belong to study protocols, not personal use instructions [1]. The same caution applies to any PE-22-28 research method, because dose and route are part of the experimental design.
A route that works in a rodent experiment does not automatically produce safe or predictable effects in humans. Without human pharmacokinetic data, pharmacodynamics, and safety monitoring, route-based claims remain uncertain [16].
Nasal Administration Claims and Bioavailability Questions
Nasal administration is often discussed for neuroactive compounds because intranasal delivery can, in some contexts, influence central nervous system exposure; however, biologic and peptide delivery through the nose depends on formulation, molecule size, stability, absorption, and study design 19. That general concept does not prove intranasal PE-22-28 is effective or safe.
Claims about PE-22-28 nasal administration should therefore be treated cautiously unless supported by direct pharmacokinetic and clinical evidence. Bioavailability questions are especially important for peptides, which can be degraded, cleared, or poorly absorbed depending on route and formulation [19].
Side Effects and Safety Profile of PE-22-28
The side effect profile of PE-22-28 is not well established in humans. No approved label or large human clinical-trial safety database was identified under this name, so absence of known adverse events should not be interpreted as proof of safety [3] [4].
What Side Effects Have Been Reported in Studies?
Spadin-related preclinical literature reported selected behavioral and mechanistic outcomes, but animal studies cannot define a full human adverse-event profile [1] [16]. For PE-22-28 specifically, reliable public human safety reporting appears limited under the exact name [2] [3].
That means common clinical questions remain unanswered: headache, nausea, sedation, mood destabilization, allergic reaction, neurologic effects, cardiovascular effects, endocrine effects, and long-term adverse events have not been adequately characterized in humans for PE-22-28.
Potential Neurologic, Mood, Sedative, and Long-Term Effects
TREK-1 is involved in neuronal excitability, and related potassium-channel biology has been linked to neuroprotection, anesthesia sensitivity, and mood-related behavior in preclinical studies [8] [9] [10]. That makes neurologic and mood-related safety monitoring especially relevant for any TREK-1-active compound.
Long-term effects remain a key unknown. A compound that affects neuron signaling, synaptic pathways, mood regulation, or potassium channel activity should not be assumed safe for repeated human use without clinical safety data.
Safety Risks, Contraindications, and Higher-Risk Groups
Because PE-22-28 lacks approved labeling, there is no regulator-reviewed contraindication list under this name. The safest approach is to treat unknown contraindications as a safety gap rather than as evidence that no contraindications exist [4] [16].
Pregnancy, Breastfeeding, Bipolar Disorder, and Epilepsy Considerations
Pregnancy and breastfeeding require special caution because fetal, neonatal, and lactation safety cannot be inferred from rodent mood models. Without approved labeling or human reproductive safety data, PE-22-28 should not be treated as having an established safety profile for these groups [4] [16].
Bipolar disorder, epilepsy, and other neurologic or psychiatric conditions also require caution. Depression guidelines emphasize clinical assessment and appropriate management, while ion-channel activity is relevant to neuronal excitability, so any investigational CNS-active peptide should be discussed with a clinician in these contexts [8] [11].
What Should Readers Discuss With a Clinician Before Peptide Therapy?
Readers considering peptide therapy discussions should focus on evidence, safety, and alternatives rather than self-experimentation. A clinician can help interpret whether a claimed intervention has human evidence, whether approved treatments are available, and whether medication interactions or psychiatric risks matter.
Practical discussion checklist:
- Current diagnosis, symptoms, and treatment goals
- History of major depressive disorder, bipolar disorder, anxiety, epilepsy, stroke, or suicidal thoughts
- Current medications, including SSRIs, SNRIs, MAOIs, stimulants, sedatives, and supplements
- Pregnancy, breastfeeding, fertility plans, or reproductive safety concerns
- Regulatory status, trial registration, and whether an approved alternative exists
- Known and unknown side effects, including mood, cognition, sedation, and neurologic effects
- Whether claims are based on approved labeling, human trials, animal studies, or anecdotes
- What to do if adverse events, mood changes, or neurologic symptoms occur
Drug Interactions and Psychiatric Medication Considerations
No reliable human drug-interaction profile was identified for PE-22-28 under this name. That is not the same as saying there are no interactions; it means interactions are not well characterized in public clinical evidence.
Could PE-22-28 Interact With Antidepressant Drugs?
Because PE-22-28 is discussed as a CNS-active, TREK-1-related peptide, combining it with antidepressant drugs would raise pharmacodynamic uncertainty. Approved antidepressant classes such as selective serotonin reuptake inhibitors, serotonin–norepinephrine reuptake inhibitors, and monoamine oxidase inhibitors have known interaction concerns that are managed clinically [12] 13.
A clinician should review current medications before any investigational peptide exposure is considered. This is especially important for people taking fluoxetine or other SSRIs, MAOIs, sedatives, stimulants, antiepileptic drugs, or multiple psychiatric medications [12] [13].
Serotonin, Dopamine, Reuptake Inhibitors, and CNS-Active Drugs
Spadin research has discussed serotonergic neurotransmission, and antidepressant medications often work through monoamine pathways such as serotonin or norepinephrine reuptake inhibition [1] [12]. That overlap does not prove PE-22-28 causes serotonin syndrome, dopamine changes, or reuptake inhibition, but it does justify caution.
The safest framing is uncertainty. Until human pharmacology is established, PE-22-28 should not be assumed compatible with antidepressant drugs, anxiolytics, antipsychotics, sleep medications, stimulants, or other CNS-active compounds.
Regulatory Status: Is PE-22-28 Peptide FDA-Approved?
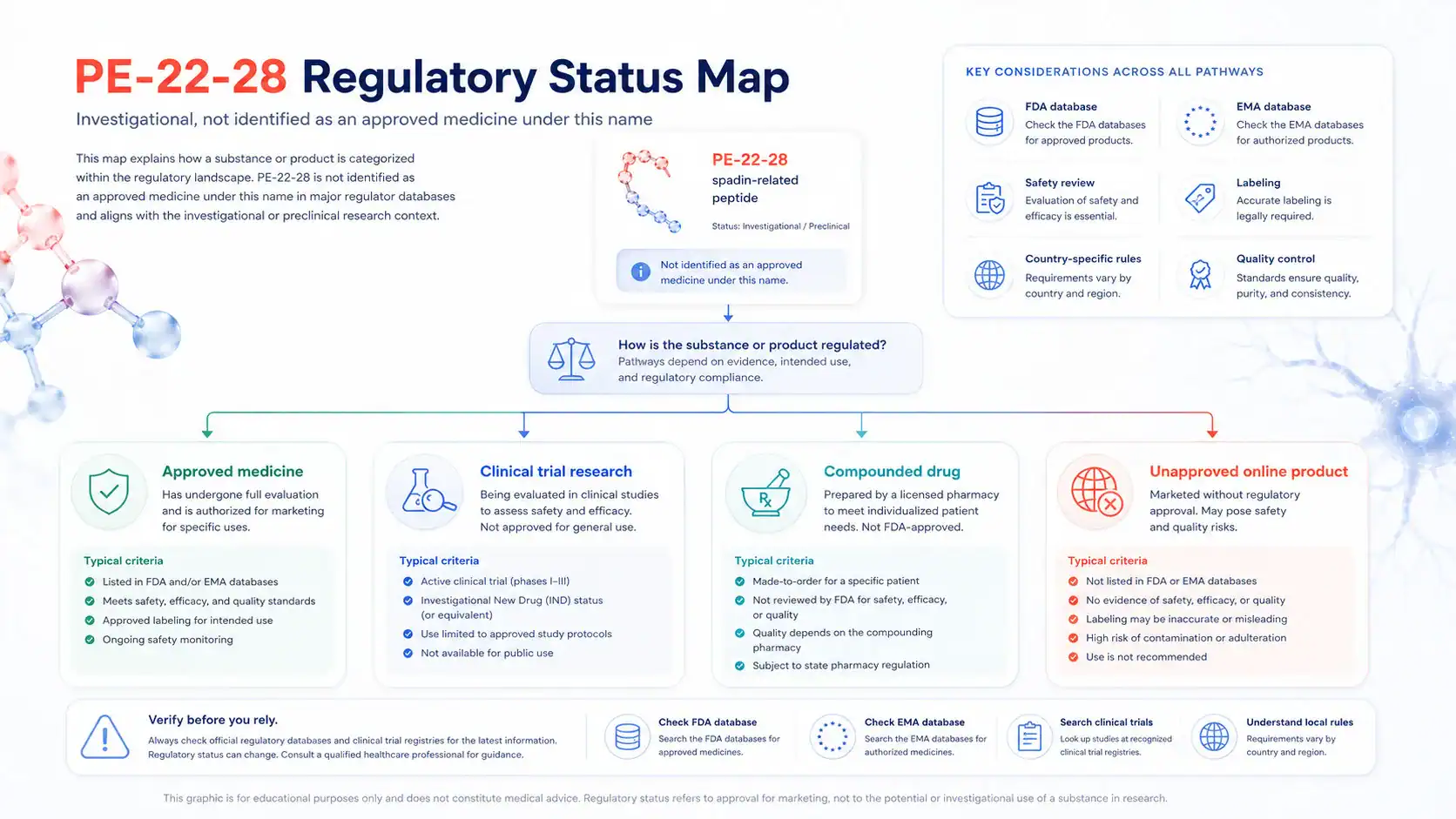
PE-22-28 peptide does not appear as an FDA-approved medicine under this name in Drugs@FDA, and it does not appear as an EMA-approved medicine under this name in the EMA medicines database [4] [5]. This means therapeutic claims should be interpreted as investigational or unsupported unless a specific approved product and indication can be verified.
Regulatory status matters because approved medicines are reviewed for manufacturing quality, labeling, dosing, safety, and efficacy for defined indications. Unapproved peptides do not have the same regulator-reviewed assurance for human use [4] 15.
Pharmaceutical-Grade PE-22-28 Claims, Compounding, and Quality Risks
Claims about “pharmaceutical-grade PE-22-28” should be evaluated carefully. FDA explains that compounded drugs are not FDA-approved, and the agency does not verify the safety, effectiveness, or quality of compounded drugs before marketing in the same way it reviews approved products 14.
Unapproved products also create quality risks, including uncertainty about identity, purity, potency, sterility, contaminants, labeling, storage, and stability. These concerns are especially relevant when online marketing claims blur the line between research chemicals and medicines [14] [15].
How Do Legal Status and Clinical Trial Rules Differ by Country?
Legal status can differ by jurisdiction, product type, intended use, compounding rules, import rules, and whether a compound is used in a regulated clinical trial. FDA and EMA databases are useful starting points, but they do not replace country-specific legal or clinical guidance [4] [5].
Clinical trials have their own registration, oversight, protocol, consent, and safety-monitoring expectations. For PE-22-28, any claim of legal therapeutic use should be verified through official regulator sources, trial registries, and a qualified healthcare professional [3] [16].
Comparison is useful only when it clarifies mechanism, evidence level, and regulatory status. It should not be used to rank peptides as “best,” imply personal use, or suggest that investigational peptides are equivalent to approved medications.
PE-22-28 Versus Spadin and Shortened Analogues
Spadin has the clearer peer-reviewed foundation, including published work describing it as a sortilin-derived peptide and TREK-1 blocker with antidepressant-like effects in rodents [1]. PE-22-28 is more narrowly discussed as a shortened spadin-related fragment or analog, with a thinner publicly visible evidence base under its exact name [2].
The practical difference is evidence depth. Spadin helps explain why PE-22-28 is scientifically interesting, but PE-22-28 still needs its own identity, pharmacology, dosing, safety, and human-outcome evidence before therapeutic claims can be considered clinically meaningful.
PE-22-28 Versus Conventional Antidepressant Medications
Conventional antidepressant medications such as SSRIs are evaluated through clinical research, approved labeling, and guideline-based care for defined patient populations [11] [12]. PE-22-28 does not have comparable approved-label or human-trial support under its name [3] [4].
That does not make conventional antidepressants risk-free, and it does not make PE-22-28 biologically irrelevant. It means the two should not be placed in the same evidence category. The safest way to interpret PE-22-28 peptide is through evidence quality, regulatory status, safety data, and clinician-guided decision-making rather than through online benefit claims or personal dosing protocols.
REFERENCES
- Mazella J, Petrault O, Lucas G, et al. Spadin, a sortilin-derived peptide, targeting rodent TREK-1 channels: a new concept in the antidepressant drug design. PLOS Biology. 2010. DOI: 10.1371/journal.pbio.1000355.
- United States National Library of Medicine. PubMed search for PE-22-28, spadin, and TREK-1 literature. PubMed database. Accessed 2026.
- U.S. National Library of Medicine. ClinicalTrials.gov search for PE-22-28. ClinicalTrials.gov. Accessed 2026.
- U.S. Food and Drug Administration. Drugs@FDA: FDA-Approved Drugs. FDA database. Accessed 2026.
- European Medicines Agency. Medicines database. EMA. Accessed 2026.
- National Center for Biotechnology Information. KCNK2 potassium two pore domain channel subfamily K member 2. NCBI Gene database. Accessed 2026.
- UniProt Consortium. KCNK2_HUMAN potassium channel subfamily K member 2. UniProtKB. Accessed 2026.
- Enyedi P, Czirják G. Molecular background of leak K+ currents: two-pore domain potassium channels. Physiological Reviews. 2010. PMID: 20393194.
- Heurteaux C, Lucas G, Guy N, et al. Deletion of the background potassium channel TREK-1 results in a depression-resistant phenotype. Nature Neuroscience. 2006. PMID: 16415869.
- Heurteaux C, Guy N, Laigle C, et al. TREK-1, a K+ channel involved in neuroprotection and general anesthesia. The EMBO Journal. 2004. PMID: 15175651.
- National Institute for Health and Care Excellence. Depression in adults: treatment and management. NICE Guideline NG222. 2022.
- Edinoff AN, Akuly HA, Hanna TA, et al. Selective Serotonin Reuptake Inhibitors. StatPearls. NCBI Bookshelf. Updated periodically.
- StatPearls Publishing. Monoamine Oxidase Inhibitors. StatPearls. NCBI Bookshelf. Updated periodically.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers. FDA. Accessed 2026.
- U.S. Food and Drug Administration. Unapproved Drugs. FDA. Accessed 2026.
- U.S. Food and Drug Administration. The drug development process: Step 3—clinical research. FDA. Accessed 2026.
- Can A, Dao DT, Arad M, Terrillion CE, Piantadosi SC, Gould TD. The mouse forced swim test. Journal of Visualized Experiments. 2012. DOI: 10.3791/3638.
- Santarelli L, Saxe M, Gross C, et al. Requirement of hippocampal neurogenesis for the behavioral effects of antidepressants. Science. 2003. PMID: 12907793.
- Lochhead JJ, Thorne RG. Intranasal delivery of biologics to the central nervous system. Advanced Drug Delivery Reviews. 2012. PMID: 22119441.
- Towfighi A, Ovbiagele B, El Husseini N, et al. Poststroke depression: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2017. PMID: 27932603.
FAQs
What is PE-22-28 peptide used for?
PE-22-28 peptide is mainly discussed as a research-stage, spadin-related peptide studied in the context of TREK-1 potassium channel biology, mood-related models, and neuroplasticity hypotheses [1]. It should not be described as an approved treatment for depression, anxiety, cognitive symptoms, or post-stroke depression. Its therapeutic use remains investigational because public human trials and approved uses have not been clearly established under the PE-22-28 name [3] [4].
How does PE-22-28 work?
PE-22-28 is thought to work through a proposed mechanism of action related to spadin and TREK-1 potassium channel modulation [1]. TREK-1 is encoded by KCNK2 and helps regulate neuronal excitability through potassium conductance [6] [7]. This mechanism may help explain research interest in effects on mood, but mechanistic plausibility does not prove clinical efficacy, cognitive enhancement, or safe human use.
What are the potential benefits of PE-22-28?
Potential benefits of PE-22-28 are best framed as preclinical or mechanistic hypotheses. Related spadin and TREK-1 research has examined antidepressant-like effects, neurogenesis, and neuroprotective pathways in animal or mechanistic studies [1] [9] [10]. Claims about mental clarity, cognitive enhancement, anxiolytic effects, or improved mood are not established clinical outcomes. Human evidence is needed before these claims can be treated as proven therapeutic benefits.
Are there human studies or clinical studies on PE-22-28?
Human studies on PE-22-28 appear absent or very limited in major public research sources under the exact PE-22-28 name [2] [3]. Most discussion comes from spadin, TREK-1, animal model, and mechanism-based research rather than large clinical studies. That means efficacy, half-life, pharmacokinetics, adverse effects, and patient outcomes are not well defined for PE-22-28 in humans.
What side effects or safety concerns are known for PE-22-28?
Side effects of PE-22-28 are not well characterized in humans because no approved label or large clinical safety database was identified under this name [3] [4]. Possible safety concerns include unknown neurologic effects, mood changes, sedation, drug interactions, allergic reaction, and long-term adverse events. People with bipolar disorder, epilepsy, pregnancy, breastfeeding, or psychiatric medication use should treat the evidence gap as a reason for clinician-supervised caution.
Is PE-22-28 FDA-approved, and what does that mean for dosage?
PE-22-28 is not identified as an FDA-approved medicine under this name, and no approved prescribing information or labeled dosage was found in FDA or EMA medicine databases [4] [5]. That means there is no regulator-reviewed recommended dosing, approved route of administration, or labeled indication. Any dosage discussion should be limited to published study context and should not be converted into personal dosing advice.
Contributing Authors
The following authors are recognized for published research that helped shape the scientific and clinical context discussed in this article.
Catherine Heurteaux
Author profile: PubMed Author Search
Catherine Heurteaux is a scientific author whose published work is directly relevant to TREK-1 potassium channel biology, preclinical research models, and mechanism-of-action discussions surrounding PE-22-28 peptide. Her publications help frame why TREK-1 became a pharmacology target of interest in mood-related research and why findings from animal models require careful interpretation. The selected papers below are especially relevant to the article’s discussion of TREK-1, potassium-channel signaling, neuroprotection, and the limits of translating preclinical findings into clinical evidence.
Selected publications:
Marc Borsotto
Author profile: PubMed Author Search
Marc Borsotto is a research author whose publications are closely connected to the spadin and TREK-1 literature discussed in this PE-22-28 peptide article. His work is relevant to understanding spadin-related peptide pharmacology, TREK-1 channel inhibition, and how preclinical findings are used to generate therapeutic hypotheses without establishing clinical efficacy. The selected publications below provide important background for interpreting PE-22-28 as an investigational, spadin-related research peptide rather than an approved therapeutic product.
Selected publications: