
PEG-MGF peptide is an investigational, PEGylated form of mechano growth factor discussed in relation to IGF-1 splice-variant biology, muscle repair, and regeneration research 3 13. This educational guide reviews what is known from molecular biology, exercise studies, preclinical models, safety literature, and regulatory databases without giving personal dosing or injection advice 1 2. Because direct human evidence for PEG-MGF therapy is very limited, claims about muscle growth and recovery should be interpreted through evidence quality rather than online popularity [2] 10.
- PEG-MGF is commonly described as a synthetic peptide designed by attaching polyethylene glycol, or PEG, to an MGF-related peptide to potentially change pharmacokinetics and half-life interpretation [13] 14.
- MGF refers to mechano growth factor, a term used in the literature for IGF-1 splice-variant biology and E-peptide research, especially in skeletal muscle adaptation and repair models [3] 5.
- Interest in PEG-MGF comes from studies of exercise-related MGF expression, satellite cells, myosatellite cell biology, and local growth-factor signaling after muscle damage 6 8 9.
- Direct clinical evidence for PEG-MGF peptide therapy is not comparable to evidence for approved peptide therapeutics, and public regulatory databases do not establish an FDA-approved PEG-MGF indication or label dose [1] [2].
- Potential benefits of MGF for muscle repair, muscle regeneration, or tissue growth are biologically plausible mainly from mechanistic, exercise, animal, and cell-model research rather than proven therapeutic outcomes in humans 7 [10].
- Side effects are not well characterized for PEG-MGF; theoretical concerns include IGF-1 pathway effects, PEG immune reactions, injection-site risks, product-quality problems, and unknown long-term safety 15 16 20.
- Dosage information should be interpreted only as regulatory or published-study context; it should not be converted into a personal dose, protocol, cycle, stack, or self-administration plan [1] 11.
Fast Answer
PEG-MGF peptide is a synthetic, PEGylated mechano growth factor–related peptide discussed for muscle repair and regeneration, but it is not an FDA-approved therapeutic drug and direct registered human trials are not evident in public ClinicalTrials.gov searches [1] [2]. Interest comes from IGF-1 splice-variant biology, exercise-related MGF expression, and satellite-cell research in skeletal muscle [3] [6] [9]. Proposed benefits are biologically plausible but not proven as human peptide therapy; dose, injection route, side effects, legality, and anti-doping status need clinician and regulatory context [16] 22.
What Is the PEG-MGF Peptide?
PEG-MGF peptide is typically discussed as a pegylated version of an MGF-related synthetic peptide, not as a conventional approved prescription drug. The key distinction is that MGF biology comes from endogenous IGF-1 gene splicing and E-peptide research, while PEG-MGF is an exogenous modified compound discussed mostly in investigational and non-approved contexts [3] [10].
Pegylated Mechano Growth Factor and Basic Peptide Structure
“Pegylated mechano growth factor” means an MGF-related peptide has been modified with polyethylene glycol. PEGylation is used in drug design to change properties such as molecular size, circulation time, renal clearance, solubility, and sometimes immune recognition, although the effect depends on the molecule and formulation [13] [14].
For PEG-MGF, the practical point is not that PEG guarantees better therapeutic effects. It only means the peptide has been chemically modified in a way that may change exposure compared with unmodified MGF, and those changes must be tested rather than assumed [13] [15].
Mechano Growth Factor as an IGF-1 C-Terminal E-Peptide
Mechano growth factor is commonly discussed as part of IGF-1 splice-variant biology, especially the IGF-1Ec-related E-peptide in humans and related MGF terminology in animal models [3]. The IGF1 gene encodes insulin-like growth factor 1, and alternative splicing can generate different transcripts that include different E-peptide regions before processing to mature IGF-1 forms [3] 4.
That matters because “MGF peptide” does not simply mean “IGF-1.” It usually refers to interest in the E-peptide region and local muscle-response biology, while the mature IGF-1 peptide has its own receptor-mediated endocrine and paracrine actions [3] [7].
Why Does PEGylation Change Half-Life Interpretation?
PEGylation often increases the apparent size of a peptide or protein, which can reduce rapid kidney filtration and extend exposure in some drug classes [13] [14]. However, PEGylation can also change tissue distribution, binding, formulation behavior, and immune recognition, so half-life assumptions for PEG-MGF cannot be treated as clinical proof [13] [15].
In other words, PEG modifies MGF-related delivery characteristics, but it does not automatically establish safety, efficacy, or a therapeutic dose. Those conclusions require product-specific pharmacokinetic, pharmacodynamic, and human safety data [13] [14].
How Does PEG-MGF Peptide Work?
The proposed mechanism centers on MGF and IGF-1-related signaling in skeletal muscle, especially local responses to mechanical stress and injury. The key limitation is that a plausible mechanism does not prove that exogenous PEG-MGF works as a human therapy [5] [10].
How Do Researchers Think PEG-MGF Works in Skeletal Muscle?
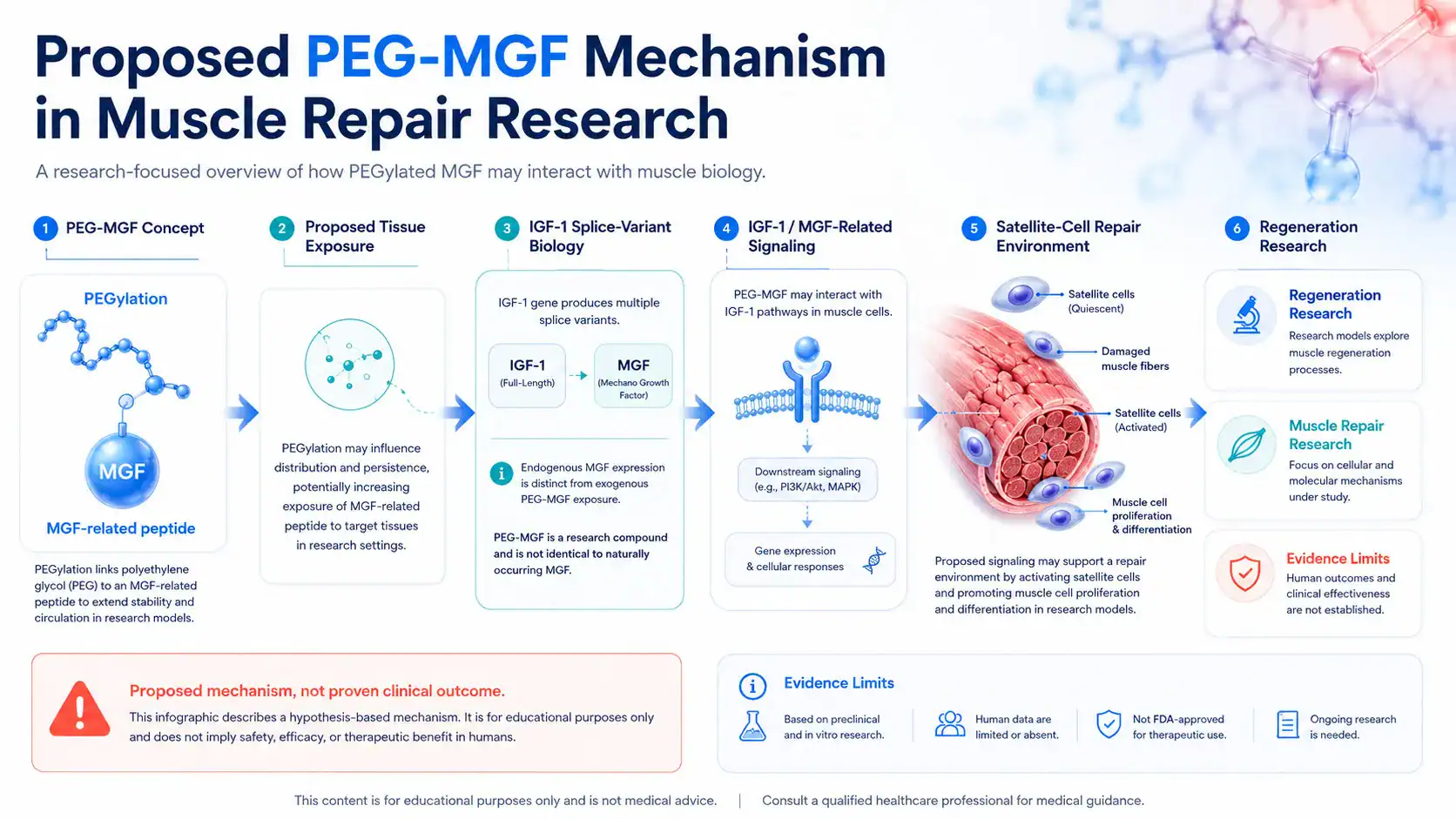
Researchers discuss MGF in the context of mechanical loading, alternative IGF-1 splicing, and local repair signals after exercise or muscle damage [5] [6]. PEG-MGF may be proposed to extend exposure to an MGF-related peptide, but direct human evidence confirming a clinically meaningful PEG-MGF mechanism in skeletal muscle is lacking [2] [10].
A safer way to phrase the mechanism is: PEG-MGF is hypothesized to influence pathways related to muscle stem cell activity, muscle cell proliferation, and growth and repair. It should not be described as proven to enhance muscle growth or accelerate recovery in humans without adequate clinical trials [10] [11].
How Might Satellite Cells Activate Muscle Stem Cell Repair?
Satellite cells, also called myosatellite cells, are skeletal muscle stem cells that support repair after injury by activating, proliferating, differentiating, and contributing to damaged muscle fibers [8] [9]. This satellite cell activation process is central to muscle regeneration biology, but many growth factors, inflammatory signals, mechanical cues, and extracellular-matrix changes are involved [8] [9].
MGF-related research is often connected to this repair environment because local IGF-1 signaling participates in muscle adaptation and regeneration [7]. That does not mean PEG-MGF directly activates satellite cells in a predictable therapeutic way in humans; it means the hypothesis fits within known muscle-biology pathways [7] [10].
What Do IGF-1 Pathways and Local MGF Expression Suggest?
IGF-1 signaling is involved in muscle protein synthesis, growth-factor signaling, and anabolic responses through pathways that include PI3K-Akt-related mechanisms, but muscle adaptation is regulated by many overlapping signals [7]. Human exercise studies have shown changes in IGF-1 splice-variant expression after resistance exercise, including MGF-related transcripts, but these studies measure endogenous response rather than administering PEG-MGF therapy [6].
This distinction is important. MGF is released or produced locally as part of the body’s response to mechanical loading, while injected or exogenous peptide therapies can have different timing, distribution, receptor exposure, and safety issues [5] [6].
PEG-MGF vs MGF: What Changes With PEGylation?
PEG-MGF vs MGF is mainly a formulation and pharmacokinetic question. The biological discussion comes from MGF and IGF-1 splice variants, while PEGylation changes how a synthetic peptide may persist or distribute [3] [13].
Why Does Native MGF Have an Extremely Short Half-Life?
Online summaries often say “MGF has an extremely short half-life,” but the clinically useful half-life of native MGF-related peptides is not standardized in approved labeling because MGF itself is not an approved drug product with a defined label pharmacokinetic profile [1] [10]. More generally, many unmodified peptides can be rapidly degraded or cleared, which is one reason PEGylation is used in peptide and protein drug development [13] [14].
The safer interpretation is that native MGF and unmodified MGF-related peptides may have limited persistence, while PEG-MGF is designed to alter that limitation. The clinical importance of that change remains unproven without PEG-MGF-specific human pharmacokinetic studies [13] [14].
How Does PEG Modify MGF and Alter Tissue Exposure?
PEG can increase hydrodynamic size and change how a peptide moves through blood and tissues [13] [14]. In some approved medicines, PEGylation has been used successfully to extend dosing intervals or improve exposure, but each PEGylated product must be evaluated on its own chemistry, target, and safety profile [13] [14].
PEG-MGF also raises product-specific unknowns, including whether the PEGylated form reaches the intended muscle tissue, how long it remains biologically active, and whether immune responses to PEG or the peptide occur [15]. Those questions are not answered by the general concept of PEGylation alone [15].
What Is PEG-MGF Peptide Used For or Studied For?
PEG-MGF is discussed online for peptide therapy for muscle, but its studied-use landscape is much narrower than marketing language suggests. It is best framed as an investigational peptide discussed around muscle repair, regeneration, and IGF-1/MGF biology rather than an approved treatment [1] [2] [10].
Where Is Muscle Repair and Regeneration Research Focused?
The research foundation focuses on skeletal muscle adaptation, satellite cells, muscle damage, local IGF-1 expression, and regeneration after injury or mechanical stress [5] [8] [9]. Human studies have examined endogenous IGF-1 splice variants after resistance exercise, while animal and cell studies have explored IGF-1 isoforms and E-peptide activity in muscle contexts [6] [11].
Applications of PEG-MGF are therefore usually inferred from this broader MGF and IGF-1 research base. That inference is scientifically interesting, but it is not the same as demonstrating that PEG-MGF therapy improves patient outcomes [10].
Why Do Muscle Growth and Recovery Claims Need Caution?
Claims about muscle growth and recovery are evidence-sensitive because they can sound like guaranteed performance or bodybuilding outcomes. In the published literature, changes in MGF expression after exercise and preclinical growth-factor experiments do not prove that exogenous PEG-MGF peptide improves lean muscle, strength, endurance, or recovery in people [6] [10] [11].
This is also where anti-doping context matters. WADA prohibits certain growth factors and related substances, including IGF-1 and analogues, in sport, so athlete use can raise regulatory and eligibility concerns beyond medical safety [22].
What Potential Benefits of MGF Peptide Therapy Are Plausible?
The potential benefits of MGF peptide therapy are best described as hypotheses or preclinical possibilities. The strongest biologic rationale involves tissue repair, muscle regeneration, satellite cells, and local growth-factor signaling, but the clinical benefit of PEG-MGF itself remains unestablished [7] [8] [10].
What Benefits of MGF for Tissue Repair Have Evidence?
MGF-related literature supports a role for local IGF-1 splice-variant responses in muscle adaptation and repair biology [3] [5]. Satellite cells are necessary for effective skeletal muscle regeneration, and growth factors can influence activation, proliferation, and differentiation in repair settings [8] [9].
What the evidence can support is biological plausibility. It cannot support the claim that PEG-MGF reliably heals injuries, repairs tissue, or restores muscle loss in humans as a proven therapy [2] [10].
Do Muscle Hypertrophy and Lean Muscle Claims Translate?
Some preclinical IGF-1 work suggests that local IGF-1 expression can affect muscle hypertrophy and regeneration in animal models 12. Other experimental work shows that different IGF-1 isoforms may produce different muscle responses, which supports the idea that splice-variant context matters [11].
Translation is the problem. Animal models, viral expression systems, and local transgene experiments are not equivalent to a human dose of a peg mgf peptide product, and they should not be treated as personal dosing evidence [11] [12].
Why “Powerful Peptide for Muscle Growth” Claims Need Caution
The phrase “powerful peptide for muscle growth” is common in promotional discussions, but it overstates the evidence if applied to human PEG-MGF outcomes. Muscle growth depends on training, nutrition, endocrine status, genetics, injury history, disease state, and many cellular pathways, not one peptide signal alone [7] [8].
A medically responsible interpretation is that PEG-MGF may be researched because MGF and IGF-1 biology are relevant to muscle. It should not be described as proven to enhance muscle, build lean muscle, or produce predictable repair and hypertrophy in people [2] [10].
What Does Human Research Say About PEG-MGF?
Human evidence is the weakest part of the PEG-MGF discussion. The most relevant human literature is mostly about endogenous MGF expression after exercise, not controlled trials of PEG-MGF peptide therapy [2] [6].
Have Direct Human Trials Evaluated PEG-MGF Peptide Therapy?
Public trial-registry evidence does not establish a robust clinical-trial program for PEG-MGF as a therapeutic drug [2]. FDA drug databases also do not identify an approved PEG-MGF product with labeled indications, safety information, or an approved dose [1].
This means direct claims about treatment, recovery, muscle repair, or disease outcomes should be treated as unproven. If future trials are registered, the key details would include population, route, formulation, dose, endpoints, adverse events, and comparator group [2].
What Do Endogenous MGF Studies After Exercise Show?
Human exercise research has reported changes in IGF-1 splice-variant expression in skeletal muscle after resistance exercise, including MGF-related transcripts [6]. These findings help explain why MGF became linked to strength training, mechanical stress, and muscle adaptation [5] [6].
But endogenous expression is not the same as administering PEG-MGF. A biopsy study showing that muscle changes its own MGF expression after exercise cannot establish that an injected synthetic peptide improves muscle growth and recovery [6] [10].
Why Bodybuilding Reports Are Not Clinical Evidence
Bodybuilding reports are anecdotal and often lack verified compound identity, dosing accuracy, adverse-event tracking, lab monitoring, and control groups. They may also involve confounders such as anabolic steroid use, growth hormone, training changes, nutrition changes, or multiple peptide therapies at once [7] [22].
Anecdotes can generate questions, but they cannot determine safety, efficacy, contraindications, or dose-response. For medical decision-making, controlled human data and regulatory review carry far more weight than online reports [1] [2].
What Does Preclinical PEG-MGF Research Suggest?
Preclinical research can help explain mechanism, but it cannot prove therapeutic benefit in humans. For PEG-MGF, much of the discussion relies on MGF, IGF-1 isoform, and muscle-regeneration models rather than PEG-MGF-specific clinical outcomes [10] [11].
What Animal Models Suggest About Growth and Repair
Animal studies have shown that local IGF-1 expression can influence skeletal muscle hypertrophy and regeneration in specific experimental systems [12]. Viral expression of IGF-1 isoforms has also been used to study different muscle responses, which supports the idea that isoform context can matter biologically [11].
These models are useful but limited. They do not define a safe PEG-MGF dose, prove therapeutic efficacy, or establish long-term safety in humans [11] [12].
What In Vitro Findings Show About Muscle Cell Proliferation
In vitro research and mechanistic reviews suggest that IGF-1 isoforms and E-peptide regions may affect muscle cell proliferation, differentiation, or repair signaling under certain experimental conditions [3] [10]. These findings are part of the reason MGF peptide therapy is discussed in regenerative medicine and tissue engineering circles [3] [10].
Cell studies are early-stage evidence. A muscle cell response in culture does not account for human pharmacokinetics, immune response, tissue targeting, disease status, or systemic safety [13] [15].
How Strong Is the Evidence for Applications of PEG-MGF?
The evidence is strongest for general muscle-biology concepts and weakest for direct PEG-MGF therapy outcomes. Separating approved use, clinical evidence, early human evidence, preclinical evidence, and unsupported claims prevents the article from turning biological plausibility into a treatment promise.
Evidence Ladder: Approved Use, Clinical, Preclinical, Unsupported
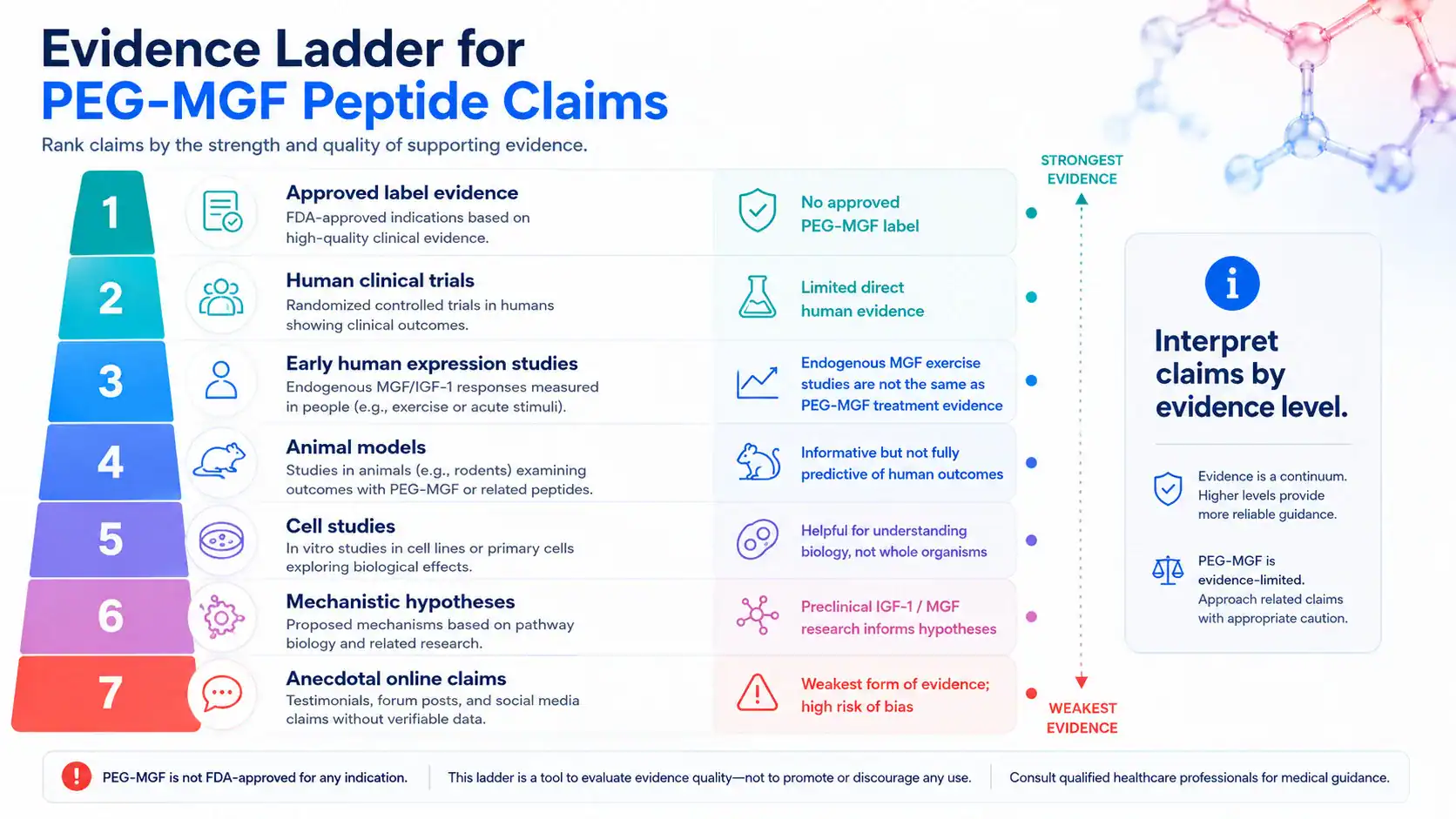
| Evidence Area | What Has Been Studied | Evidence Level | What It Can and Cannot Show |
|---|---|---|---|
| FDA-approved PEG-MGF use | No FDA-approved PEG-MGF product or label dose is established in Drugs@FDA review context [1]. | Approved use: not established | Can clarify regulatory status; cannot support therapeutic use. |
| Direct PEG-MGF human trials | Public trial-registry review does not establish direct PEG-MGF therapeutic trials as a mature evidence base [2]. | Clinical evidence: not established | Can show evidence gaps; cannot prove benefit or safety. |
| Endogenous MGF after exercise | Resistance exercise studies have measured IGF-1 splice variants in human skeletal muscle [6]. | Early human evidence | Can support biological relevance; cannot prove exogenous PEG-MGF therapy works. |
| IGF-1 isoform animal models | Local or viral IGF-1 isoform work has examined hypertrophy and regeneration in animals [11] [12]. | Preclinical | Can explore mechanisms; cannot define human treatment effects. |
| Satellite-cell biology | Satellite cells drive muscle regeneration after injury [8] [9]. | Mechanistic/preclinical and human biology | Can explain repair pathways; cannot prove a peptide intervention works. |
| Online muscle-growth claims | Promotional or bodybuilding claims often exceed controlled evidence and may overlap with anti-doping concerns [22]. | Unsupported/anecdotal | Can identify popular claims; cannot establish medical use. |
Claim Strength Matrix for Muscle Repair and Regeneration
For muscle repair, the evidence is biologically plausible but not clinically proven for PEG-MGF. The claim is supported by satellite-cell and IGF-1 pathway biology, but it lacks adequate human treatment trials [8] [9] [10].
For muscle hypertrophy, the claim is weaker when applied to people using PEG-MGF. Animal and viral-expression models can show possible mechanisms, but they do not translate into a validated human peptide therapy protocol [11] [12].
For regeneration after injury or myopathy, the claim remains investigational. Muscle-loss states can involve inflammation, denervation, disuse, endocrine disease, aging, or genetic myopathy, so a growth-factor hypothesis cannot replace diagnosis or evidence-based care [7] [8].
Source Quality Filter for PEG-MGF Research Claims
Use this filter when reading PEG-MGF research claims:
- Prefer regulator databases, clinical-trial registries, peer-reviewed human studies, and mechanistic reviews over sales pages [1] [2].
- Separate endogenous MGF expression from exogenous PEG-MGF administration [6] [10].
- Separate animal, cell, and tissue-engineering findings from human outcomes [11] [12].
- Check whether the compound is PEG-MGF, native MGF, mature IGF-1, an IGF-1 isoform, or another peptide therapy [3] [13].
- Treat dose, injection route, and product purity claims cautiously unless they come from labeling or peer-reviewed study methods [16] [17].
Side Effects of PEG-MGF Peptide: What Is Known?

Side effects of PEG-MGF are not well defined because there is no approved label and limited direct human clinical evidence. Safety discussion therefore relies on uncertainty, general peptide-injection risks, PEGylation literature, and cautious comparison to IGF-1 pathway medicines [1] [15] 19.
What Side Effects Are Reported or Theoretically Plausible?
Because PEG-MGF lacks an approved prescribing label, there is no regulator-reviewed adverse-reaction table for a standardized product [1]. Theoretical risks include local reactions, immune reactions to peptide or PEG components, fluid or glucose-related effects through growth-factor pathways, and unknown effects on abnormal tissue growth [15] [19] [20].
Approved recombinant IGF-1 products such as mecasermin are not the same as PEG-MGF, but their labels and regulator summaries show that IGF-1 pathway drugs can have clinically important risks and specialist-use restrictions [19]. Those risks should not be copied directly onto PEG-MGF, but they are relevant caution signals for clinician discussion [19].
Injection-Site Reactions and Product-Quality Concerns
Any injection-based administration route can introduce risks such as pain, irritation, infection, contamination, or improper handling when sterile technique and regulated manufacturing controls are absent 18. This article does not provide injection instructions, mixing instructions, or reconstitution steps.
Quality-control concerns are especially important for unapproved or compounded peptides. FDA explains that compounded drugs are not FDA-approved in the same way as approved medicines, and unapproved drugs may lack evidence of safety, effectiveness, quality, and labeling adequacy [16] 17.
What Long-Term Safety Gaps Remain Unknown?
Long-term PEG-MGF safety is unknown because sustained human exposure has not been characterized in approved labeling or robust clinical trials [1] [2]. Key gaps include immune response, metabolic effects, repeated-exposure risks, tissue selectivity, fertility and pregnancy safety, cancer-related concerns, and interactions with other anabolic or endocrine agents [15] [20].
IGF-1 signaling is biologically involved in cell growth and survival, and epidemiologic and mechanistic literature has examined associations between IGF signaling and cancer risk [20] 21. Those data do not prove PEG-MGF causes cancer, but they support caution around unsupervised growth-factor manipulation [20] [21].
Safety Risks, Contraindications, and Medical Supervision
Contraindications for PEG-MGF are not defined in an approved label because there is no approved PEG-MGF prescribing information. In practice, that absence increases uncertainty rather than reducing risk [1] [17].
Which Groups Need Extra Caution or Avoidance?
Extra caution is reasonable for people who are pregnant or breastfeeding, minors, people with active or prior cancer, diabetes or glucose disorders, endocrine disease, unexplained swelling, active infection, or significant heart, liver, or kidney disease. These groups are commonly more vulnerable to unknown drug effects, and IGF-1 pathway medicines require specialist evaluation in approved contexts [19] [20].
Athletes also need extra caution because growth-factor-related substances can create anti-doping violations even when a product is marketed as a peptide or research compound [22]. Legal eligibility and medical safety are separate issues, and both need authoritative verification [22].
Cancer, Abnormal Tissue Growth, and IGF-1 Pathway Concerns
IGF-1 signaling participates in growth, metabolism, survival signaling, and tissue responses, which is why it is relevant to both muscle biology and oncology research [7] [20]. Reviews and meta-analyses have examined relationships between circulating IGF-1, IGF-binding proteins, and cancer risk across populations, although such evidence does not establish PEG-MGF-specific causation [20] [21].
The safety concern is mechanistic uncertainty. A peptide discussed for tissue growth or regeneration should not be assumed harmless, especially when long-term human exposure, tissue selectivity, and dose-response are not established [15] [20].
Drug Interactions With Growth Hormone or Anabolic Agents
Direct PEG-MGF drug-interaction studies are not established in approved labeling or mature clinical trials [1] [2]. Theoretical concerns include overlapping effects with growth hormone, recombinant IGF-1, anabolic steroids, insulin or glucose-lowering drugs, and other peptide therapies affecting growth, glucose, or tissue signaling [7] [19].
This is not a “stacking” recommendation. It is a safety reason to discuss current medications, supplements, hormone therapies, and performance-enhancing substances with a licensed clinician [19] [22].
What Dosage Information Exists for PEG-MGF Peptide?
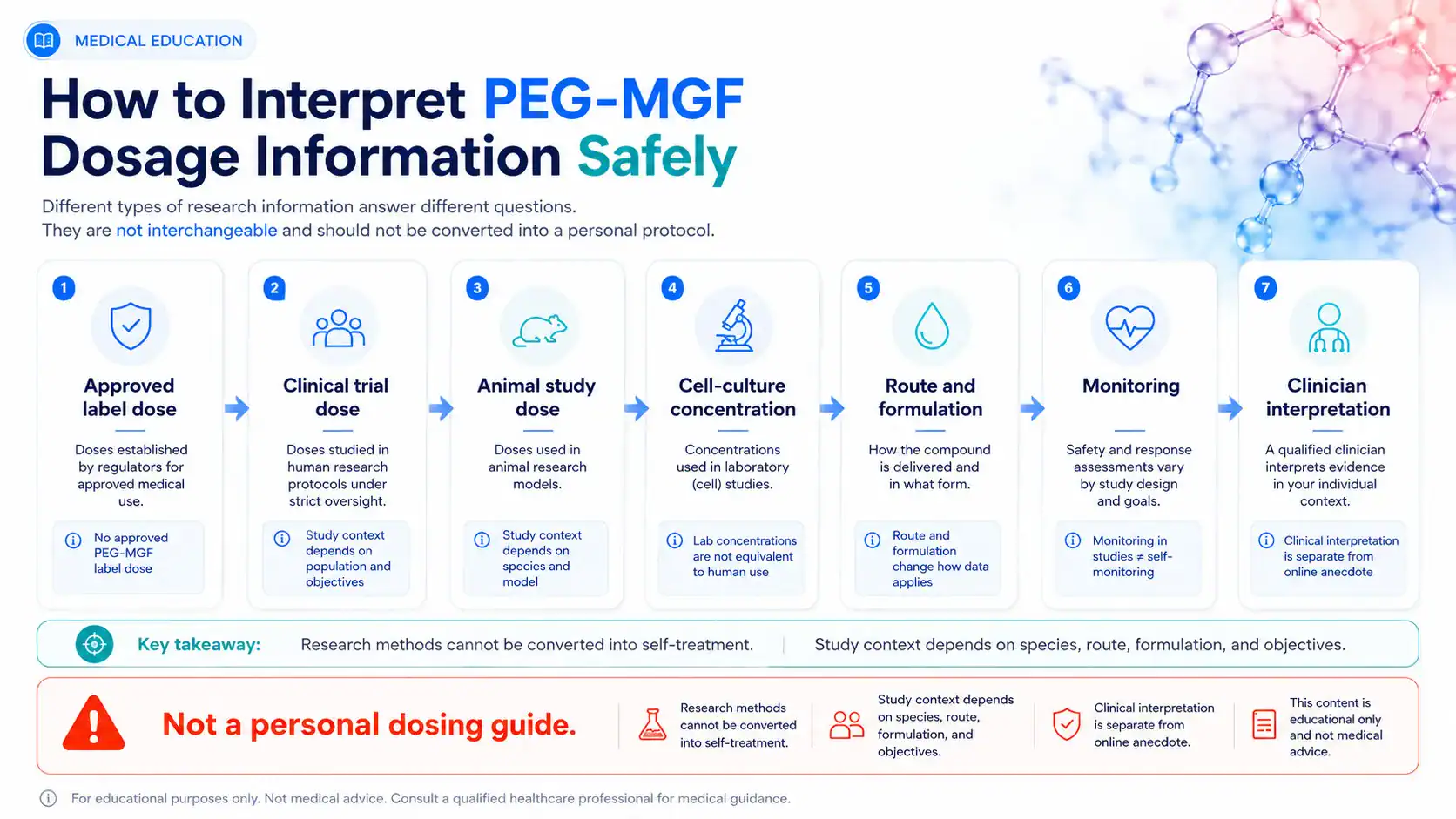
There is no approved PEG-MGF dosage for therapeutic use in FDA labeling. Dosage information in this article is therefore limited to evidence context and should not be interpreted as personal medical advice [1].
No Approved Label Dose for PEG-MGF
Drugs@FDA does not establish an approved PEG-MGF label, indication, route, dosing schedule, contraindication list, or adverse-reaction table [1]. That means there is no regulator-reviewed “best dose,” “beginner dose,” “cycle,” or “protocol” for PEG-MGF peptide.
This is a major difference from approved medicines. Approved products have specific manufacturing standards, indications, dosage instructions, contraindications, warnings, and adverse-event information reviewed for the labeled use [1] [17].
Study Dose Ranges Versus Personal Dosing Advice
Published muscle-biology studies often involve exercise biopsies, endogenous mRNA expression, cell culture, animal models, local transgene expression, or viral expression systems rather than a standardized PEG-MGF human dose [6] [11] [12]. These methods cannot be converted into a personal dose because species, route, formulation, exposure, disease state, and endpoints differ [11] [12].
Study doses should not be interpreted as personal dosing advice. Any future dose discussion would need to specify the exact compound, formulation, PEG size, route, trial population, monitoring plan, and adverse-event data [13] [15].
What Administration Routes Are Discussed in the Literature?
Administration routes discussed around MGF-related research vary by study type. Human exercise studies may measure endogenous expression after resistance training, while animal and cell models may use experimental delivery systems that are not clinical instructions [6] [11] [12].
Injection Routes in Research Settings, Not Self-Administration Guidance
PEG-MGF is often discussed online in relation to injection, but there is no approved PEG-MGF label that provides a medically reviewed injection route or self-administration protocol [1]. Research delivery methods are study procedures, not instructions for personal use [11] [12].
Route matters because it changes pharmacokinetics, local tissue exposure, systemic exposure, immune risk, and adverse-event monitoring [13] [15]. For safety, injection-related decisions should remain within regulated clinical or research settings, and this article does not provide step-by-step administration guidance [18].
Is PEG-MGF Legal or FDA-Approved?
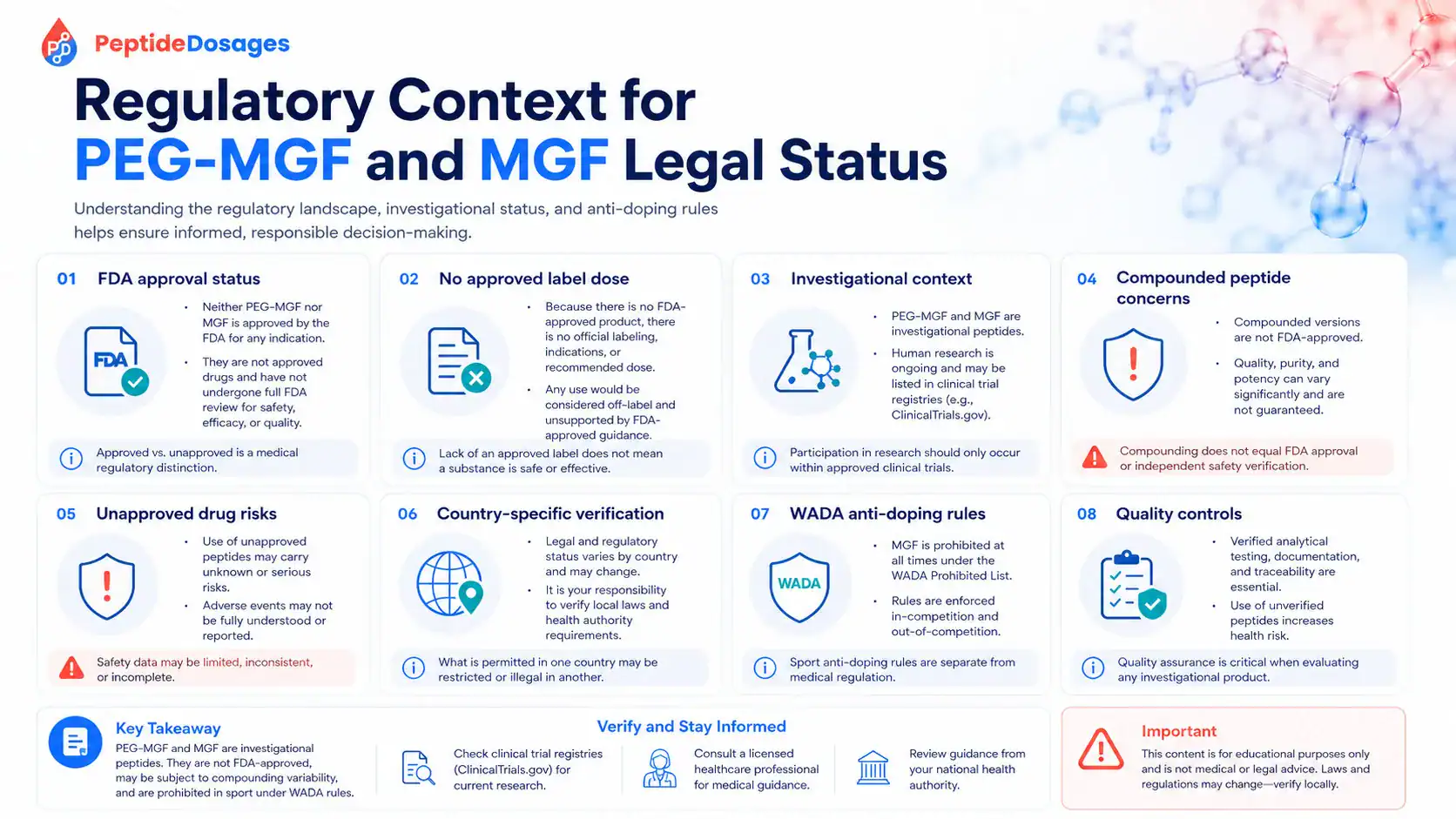
PEG-MGF legal status depends on jurisdiction, product claims, intended use, compounding rules, sport regulations, and whether a product is being marketed for human therapeutic use. In the United States, the central medical point is that PEG-MGF is not established as an FDA-approved drug with labeled indications or dosage information [1].
FDA Approval Status and Investigational-Drug Context
FDA approval status matters because approved drugs are reviewed for a specific product, indication, dose, route, labeling, manufacturing quality, and safety profile [1]. PEG-MGF does not have that kind of approved FDA therapeutic label in the public FDA drug database context [1].
If PEG-MGF were studied as an investigational drug, trial oversight, informed consent, manufacturing controls, safety monitoring, and regulatory submissions would be central. Public trial-registry review is the appropriate starting point for checking whether controlled human studies exist or are recruiting [2].
MGF Legal Status, Compounding, and Quality-Control Concerns
MGF legal status should not be reduced to a simple internet yes-or-no answer. FDA distinguishes approved drugs from compounded and unapproved drugs, and compounded products are not FDA-approved for safety, effectiveness, or manufacturing quality before marketing [16] [17].
That distinction matters for any use of PEG-MGF. Product identity, purity, sterility, dose accuracy, storage, labeling, and adverse-event reporting can differ greatly outside approved-drug systems [16] [17].
Athlete and Anti-Doping Considerations for IGF-1 Analogs
Athletes should also consider anti-doping rules. WADA’s Prohibited List includes growth factors and related substances such as IGF-1 and analogues under prohibited categories, and athletes are responsible for substances found in their bodies [22].
A peptide may be unapproved medically and prohibited in sport at the same time. Regulatory legality, anti-doping eligibility, and medical safety are different questions that require separate verification [22].
How Does PEG-MGF Compare With Related Peptide Therapies?
PEG-MGF is best compared by mechanism, evidence level, and regulatory status rather than by claims about “best” outcomes. The most relevant comparisons are native MGF or MGF E-peptide concepts, mature IGF-1 or mecasermin, and broader growth hormone/IGF-1 axis therapies [3] [7] [19].
PEG-MGF vs MGF and Related IGF-1 Approaches
| Compound or Approach | Main Concept | Evidence and Regulatory Context | Key Safety Interpretation |
|---|---|---|---|
| PEG-MGF | PEGylated MGF-related synthetic peptide intended to alter exposure [13] [14]. | No FDA-approved PEG-MGF label or established therapeutic dose [1]. | Safety and efficacy remain uncertain; do not treat as an approved therapy. |
| Native MGF / MGF E-peptide | IGF-1 splice-variant and C-terminal E-peptide biology [3] [10]. | Human exercise and mechanistic literature support biological relevance [5] [6]. | Endogenous expression does not prove benefit from external peptide use. |
| Recombinant human IGF-1, such as mecasermin | Approved IGF-1 medicine for specific severe IGF-1 deficiency contexts in some jurisdictions [19]. | Has regulator-reviewed product information and specialist-use restrictions [19]. | Not interchangeable with PEG-MGF; shows why growth-factor drugs require monitoring. |
| Growth hormone / GH-IGF axis approaches | Endocrine pathway that can influence IGF-1 and muscle metabolism [7]. | Approved uses depend on product, indication, age, diagnosis, and jurisdiction [1] [7]. | Interaction and misuse risks require clinician oversight and anti-doping awareness [22]. |
Key Takeaways Before Readers Consider MGF With a Clinician
Before considering MGF, PEG-MGF, or related peptide therapies with a licensed clinician, useful discussion points include:
- Whether the goal is muscle repair, muscle loss evaluation, injury recovery, endocrine assessment, or athletic performance, because each requires a different evidence standard [7] [8].
- Whether the compound has an approved indication, label dose, safety profile, and regulated manufacturing pathway [1] [17].
- Whether human studies support the intended use, or whether the claim comes from preclinical, mechanistic, or anecdotal evidence [2] [10].
- Whether medical history includes cancer risk, diabetes, endocrine disease, pregnancy, breastfeeding, active infection, or unexplained symptoms [19] [20].
- Whether current medications include growth hormone, insulin, glucose-lowering drugs, anabolic agents, or other peptide therapeutics [7] [19].
- Whether sport rules, employment testing, or anti-doping regulations apply [22].
- Whether approved alternatives, physical therapy, nutrition, resistance training, rehabilitation, or disease-specific treatments have stronger evidence [7] [8].
The safest way to interpret PEG-MGF peptide is through evidence quality, regulatory status, safety data, and clinician-guided decision-making. The strongest conclusions come from approved labeling and well-designed human studies; weaker claims about muscle growth, regeneration, dose, injection, or performance should be treated cautiously.
REFERENCES
- U.S. Food and Drug Administration. Drugs@FDA: FDA-Approved Drugs Database. FDA official database. Updated continuously.
- National Library of Medicine. ClinicalTrials.gov search results for “PEG-MGF”. ClinicalTrials.gov public registry and results database. Updated continuously.
- Philippou A, Maridaki M, Pneumaticos S, Koutsilieris M. The complexity of the IGF1 gene splicing, posttranslational modification and bioactivity. Molecular Medicine. 2014. DOI: 10.2119/molmed.2014.00011.
- National Center for Biotechnology Information. IGF1 insulin like growth factor 1 [Homo sapiens]. NCBI Gene. Updated continuously.
- Goldspink G. Mechanical signals, IGF-I gene splicing, and muscle adaptation. Physiology. 2005. DOI: 10.1152/physiol.00004.2005.
- Hameed M, Orrell RW, Cobbold M, Goldspink G, Harridge SDR. Expression of IGF-I splice variants in young and old human skeletal muscle after high resistance exercise. The Journal of Physiology. 2003. DOI: 10.1113/jphysiol.2002.032136.
- Velloso CP. Regulation of muscle mass by growth hormone and IGF-I. British Journal of Pharmacology. 2008. DOI: 10.1038/bjp.2008.153.
- Charge SBP, Rudnicki MA. Cellular and molecular regulation of muscle regeneration. Physiological Reviews. 2004. DOI: 10.1152/physrev.00019.2003.
- Dumont NA, Bentzinger CF, Sincennes MC, Rudnicki MA. Satellite Cells and Skeletal Muscle Regeneration. Comprehensive Physiology. 2015. DOI: 10.1002/cphy.c140068.
- Matheny RW Jr, Nindl BC, Adamo ML. Mechano-growth factor: a putative product of IGF-I gene expression involved in tissue repair and regeneration. Endocrinology. 2010. PubMed indexed record.
- Barton ER. Viral expression of insulin-like growth factor-I isoforms promotes different responses in skeletal muscle. Journal of Applied Physiology. 2006. DOI: 10.1152/japplphysiol.01455.2005.
- Musarò A, McCullagh K, Paul A, et al. Localized Igf-1 transgene expression sustains hypertrophy and regeneration in senescent skeletal muscle. Nature Genetics. 2001. DOI: 10.1038/84839.
- Harris JM, Chess RB. Effect of pegylation on pharmaceuticals. Nature Reviews Drug Discovery. 2003. DOI: 10.1038/nrd1033.
- Veronese FM, Pasut G. PEGylation, successful approach to drug delivery. Drug Discovery Today. 2005. DOI: 10.1016/S1359-6446(05)03575-0.
- Kozma GT, Shimizu T, Ishida T, Szebeni J. Anti-PEG antibodies: Properties, formation, testing and role in adverse immune reactions to PEGylated nano-biopharmaceuticals. Advanced Drug Delivery Reviews. 2020. DOI: 10.1016/j.addr.2020.07.024.
- U.S. Food and Drug Administration. Human Drug Compounding. FDA official source. Updated continuously.
- U.S. Food and Drug Administration. Unapproved Drugs. FDA official source. Updated continuously.
- Centers for Disease Control and Prevention. Injection Safety. CDC official source. Updated continuously.
- European Medicines Agency. Increlex: European public assessment report overview. EMA official medicine information. Updated continuously.
- Pollak M. Insulin and insulin-like growth factor signalling in neoplasia. Nature Reviews Cancer. 2008. DOI: 10.1038/nrc2536.
- Renehan AG, Zwahlen M, Minder C, O’Dwyer ST, Shalet SM, Egger M. Insulin-like growth factor (IGF)-I, IGF binding protein-3, and cancer risk: systematic review and meta-regression analysis. The Lancet. 2004. DOI: 10.1016/S0140-6736(04)16044-3.
- World Anti-Doping Agency. The Prohibited List. WADA official source. Updated annually.
FAQs
What is PEG-MGF peptide?
PEG-MGF peptide is a PEGylated, MGF-related synthetic peptide discussed in relation to mechano growth factor and IGF-1 splice-variant biology. MGF is often described as an IGF-1-related E-peptide concept connected to local skeletal muscle responses, while PEGylation is intended to change properties such as exposure or half-life interpretation [3] [13]. It should be viewed as an investigational research topic, not an FDA-approved therapeutic peptide [1].
Does PEG-MGF actually work for muscle growth and recovery?
PEG-MGF has not been proven to work for muscle growth and recovery in high-quality human clinical trials. The biologic rationale comes from early human exercise studies of endogenous MGF expression and preclinical research on IGF-1-related effects on muscle [6] [11]. That evidence can support mechanistic interest, but it does not establish clinical efficacy, predictable patient outcomes, or reliable recovery benefits from PEG-MGF peptide therapy [2].
Can PEG-MGF help with injury recovery or healing?
PEG-MGF has not been established as a proven treatment for injury recovery or healing. Muscle repair and regeneration claims are mainly based on mechanistic hypotheses, satellite-cell biology, and preclinical growth-factor research rather than direct clinical evidence for PEG-MGF in injured patients [8] [9] [10]. Preclinical findings may help researchers study tissue repair pathways, but they should not be interpreted as proof of human benefit.
What adverse effects or allergic reactions are possible with PEG-MGF?
Adverse effects of PEG-MGF are not well characterized because there is no approved label with a regulator-reviewed side-effect table [1]. Possible concerns include injection-site reactions, allergic reaction risk, immune responses to PEGylated compounds, product-quality problems, and theoretical IGF-1 pathway effects [15] [18] [19]. Serious side effects and long-term safety risks remain uncertain, especially for unapproved or compounded peptide products [16] [17].
What dosage or route of administration information exists for PEG-MGF?
Dosage information for PEG-MGF should be treated as evidence context, not personal dosing advice. There is no approved label dose, and public regulatory sources do not establish a standardized clinical-trial dosage for therapeutic PEG-MGF use [1] [2]. Research may discuss experimental delivery methods or route of administration in animal, cell, or exercise-study contexts, but those methods should not be converted into self-use instructions [6] [11] [12].
Is PEG-MGF legal or approved for clinical use?
PEG-MGF is not established as FDA-approved for clinical use with a labeled indication, dose, or safety profile [1]. Legal status can depend on jurisdiction, intended use, product claims, compounding rules, and whether a product is marketed for human use [16] [17]. Athletes also need separate anti-doping review because growth-factor-related substances, including IGF-1 analogues, may fall under prohibited categories [22].
Contributing Authors
The following authors are recognized for published research that helped shape the scientific and clinical context discussed in this article.
Geoffrey Goldspink
Author profile: PubMed Author Search
Geoffrey Goldspink’s published work is closely tied to the scientific background behind mechano growth factor, IGF-1 splice-variant biology, and muscle adaptation after mechanical loading. His research helped frame how local gene expression responses in skeletal muscle became part of the broader published literature on MGF, exercise, and repair signaling. For an evidence-focused discussion of PEG-MGF peptide, these publications are useful because they help separate endogenous MGF biology from claims about exogenous PEGylated peptide use, while also showing why mechanism-of-action questions remain central to interpretation.
Selected publications:
- Mechanical signals, IGF-I gene splicing, and muscle adaptation — Physiology, 2005. DOI: 10.1152/physiol.00004.2005.
- Expression of IGF-I splice variants in young and old human skeletal muscle after high resistance exercise — The Journal of Physiology, 2003. DOI: 10.1113/jphysiol.2002.032136.
Michael A. Rudnicki
Author profile: PubMed Author Search
Michael A. Rudnicki’s publications are relevant to the muscle-regeneration context discussed in this article, especially the biology of satellite cells and skeletal muscle repair. His work provides foundational background for understanding why MGF-related pathways are often discussed alongside muscle stem cell activity, tissue repair models, and regeneration research. These publications do not establish PEG-MGF as a proven clinical therapy, but they provide important scientific context for interpreting preclinical research, evidence limitations, and the difference between cellular repair mechanisms and validated human outcomes.
Selected publications:
- Cellular and molecular regulation of muscle regeneration — Physiological Reviews, 2004. DOI: 10.1152/physrev.00019.2003.
- Satellite Cells and Skeletal Muscle Regeneration — Comprehensive Physiology, 2015. DOI: 10.1002/cphy.c140068.