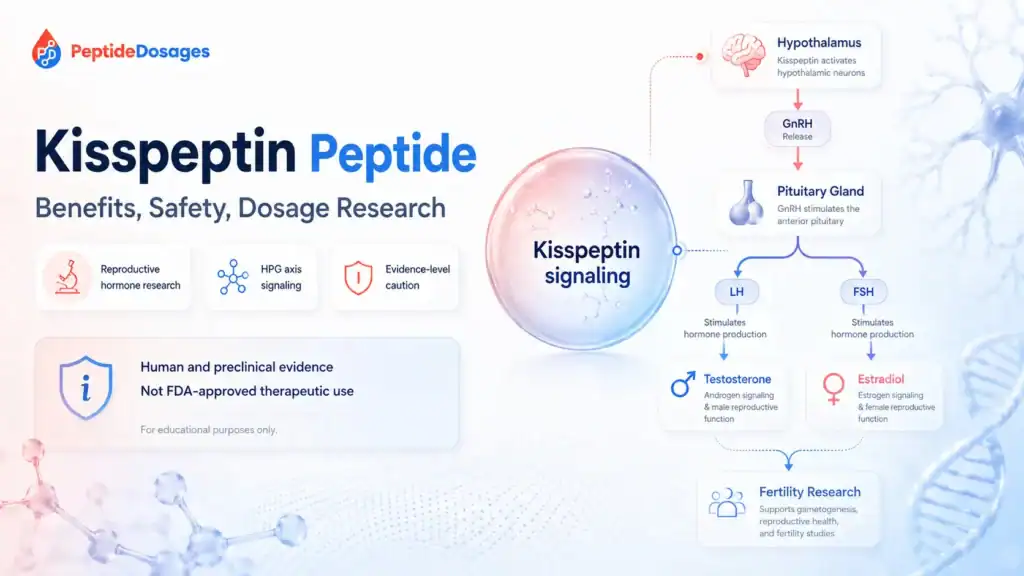
Kisspeptin peptide is a naturally occurring reproductive neuropeptide system best known for helping regulate gonadotropin-releasing hormone, or GnRH, and the hypothalamic-pituitary-gonadal axis.1 It is discussed in fertility, puberty, reproductive hormone, and endocrine research because kisspeptin signaling can stimulate downstream luteinizing hormone and follicle-stimulating hormone release in controlled human and animal studies.2 This educational article reviews the evidence, safety questions, dosage information from published studies, and regulatory status without providing personalized medical advice.
- Kisspeptin refers to a family of peptides encoded by the KISS1 gene; kisspeptin-10 is the shortest biologically active C-terminal fragment commonly studied in research.[1]
- Kisspeptin and its receptor, historically called GPR54 and now commonly known as KISS1R, are central to reproductive hormone signaling.23
- Human studies have examined kisspeptin administration for LH release, reproductive hormone secretion, and assisted reproduction settings, but evidence remains early and context-specific.45
- Potential benefits of kisspeptin are most plausible where they align with GnRH, LH, FSH, ovulation, or sex steroid biology, but they should not be treated as proven general health claims.6
- Safety data come mainly from small or specialized clinical studies, so long-term safety, repeated-use risks, and unapproved-product quality remain important uncertainties.[5]7
- Study dosing has used medically supervised research protocols, including intravenous and subcutaneous administration, and should not be converted into personal dosing advice.[4][5]
- Kisspeptin peptide is not listed as an FDA-approved drug product for routine therapeutic use in the United States, and investigational or compounded contexts require careful regulatory interpretation.89
Fast Answer
Kisspeptin peptide is a reproductive hormone-signaling peptide that helps stimulate GnRH neurons and downstream LH and FSH release through the kisspeptin receptor.[2][6] People search for it because of fertility, puberty, testosterone, libido, and reproductive health research, but most uses remain investigational rather than approved medical indications.[8][9] Human evidence exists, especially in controlled endocrine and assisted reproduction studies, yet dosage, safety, and administration findings should be interpreted as research context, not personal medical guidance.[4][5]
What Is the Kisspeptin Peptide?
Kisspeptin is not a single consumer “peptide therapy” product. It is a family of related peptides produced from the KISS1 gene, including longer kisspeptin forms and shorter fragments such as kisspeptin-10.[1][2] These peptides bind the kisspeptin receptor, KISS1R, a G protein-coupled receptor involved in reproductive endocrine signaling.[2][3]
The term kisspeptin peptide often appears in searches about fertility, hormone release, puberty, testosterone, and reproductive function. That interest is biologically understandable, but it needs evidence grading: some findings come from human endocrine studies, while others come from animal, cell, or mechanistic work.[6]10
Kisspeptin as a Reproductive Hormone Signal
Kisspeptin is best understood as a signal upstream of GnRH. GnRH is released from the hypothalamus and acts on the pituitary gland, which then releases luteinizing hormone and follicle-stimulating hormone.[6][10] LH and FSH help regulate ovarian and testicular function, including ovulation, testosterone production, estradiol production, and gamete development.[6]
This makes kisspeptin a key part of the reproductive axis rather than a broad, proven wellness peptide. Its strongest scientific relevance is in reproductive endocrinology, not generalized anti-aging, performance, or vitality claims.[6][10]
Kisspeptin-10 and Other Kisspeptin-Derived Peptide Fragments
Kisspeptin-10 is a 10-amino-acid fragment that contains the core active region needed to activate the kisspeptin receptor.[1][2] Longer forms such as kisspeptin-54 have also been studied in humans, including fertility and endocrine research settings.[4][5]
The differences between kisspeptin-10 and kisspeptin-54 matter because peptide length can influence pharmacokinetics, receptor activation duration, study design, and administration route.[1][4] A finding with one kisspeptin fragment should not automatically be assumed to apply to all kisspeptin-derived peptides.
Why Kisspeptin Is Discussed in Fertility and Endocrine Research
Kisspeptin became central to reproductive biology after human genetic studies linked loss-of-function changes in GPR54/KISS1R to hypogonadotropic hypogonadism and impaired puberty.1112 These findings helped show that kisspeptin signaling is not just a laboratory curiosity; it is required for normal activation of the reproductive axis.[11][12]
Researchers have since studied kisspeptin administration as a way to stimulate endogenous GnRH and gonadotropin release. That approach differs from giving downstream hormones directly, but it remains mostly investigational outside research settings.[5][9]
How Does Kisspeptin Peptide Work in the Reproductive Axis?
Kisspeptin works mainly by activating kisspeptin receptors on or near GnRH neurons in the hypothalamus.[6][10] This can stimulate GnRH release, which then promotes pituitary release of LH and FSH.[6] The effect is upstream, meaning kisspeptin may influence the body’s own reproductive hormone signaling rather than simply replacing a hormone.
This mechanism is biologically plausible and well supported in reproductive neuroendocrinology. Still, mechanism does not equal clinical effectiveness for every claimed use.[6][10]
The Hypothalamus, GnRH Release, and Pituitary Hormone Release
The hypothalamus acts as a control center for reproductive hormone timing. Kisspeptin neurons provide stimulatory input to GnRH neurons, and GnRH then signals the pituitary gland to release LH and FSH.[6][10]
LH can stimulate testosterone production in the testicle and support ovulation-related processes in the ovary, while FSH supports follicular development and spermatogenesis.[6] This explains why researchers measure LH, FSH, testosterone, estradiol, and menstrual cycle markers when studying the effects of kisspeptin.[4][5]
Kisspeptin Receptor Activity and G Protein-Coupled Receptor Signaling
The kisspeptin receptor is a G protein-coupled receptor originally identified in metastasis and reproductive biology research.[2][3] Activation of this receptor can trigger intracellular signaling pathways that increase GnRH neuron activity and reproductive hormone secretion.[6][10]
The phrase “kisspeptin stimulates hormones” is accurate only in a specific biological sense. Kisspeptin can stimulate GnRH-related hormone release in controlled settings, but the size, duration, and clinical meaning of that response depend on peptide form, dose, route, population, and baseline endocrine status.[4][6]
Why Kisspeptin Signaling Does Not Always Predict Clinical Outcomes
A receptor response is not the same as a therapeutic outcome. A short-term rise in LH does not prove improved fertility, normalized puberty, restored testosterone, or better sexual function in all populations.[6][10]
Clinical outcomes depend on many factors, including ovarian reserve, hypothalamic function, pituitary responsiveness, sex steroid feedback, metabolic health, and underlying diagnosis.[5][7] This is why kisspeptin research should be read through evidence level, not just mechanism.
The Role of Kisspeptin Neurons in Puberty and Reproduction
Kisspeptin neurons are important regulators of reproductive maturation and ongoing reproductive function.[6][10] They integrate signals from sex steroids, metabolic state, and other neuroendocrine pathways.
This role makes kisspeptin relevant to puberty research, menstrual cycle biology, ovulation, fertility, and hypogonadotropic hypogonadism. It also makes inappropriate self-directed use risky, because altering reproductive hormone signaling can have broad endocrine effects.[6][11]
How Kisspeptin Neurons Help Regulate Onset of Puberty
Human genetic studies showed that disrupted KISS1R signaling can cause failure of normal puberty and isolated hypogonadotropic hypogonadism.[11][12] These findings support a role for kisspeptin signaling in the onset of puberty.
The reverse has also been explored: increased or altered kisspeptin signaling has been investigated in relation to puberty timing, including precocious puberty research, but this does not establish kisspeptin as a self-directed treatment for puberty disorders.[10]13
Sex Steroid Feedback, Testosterone, and Estradiol Signaling
Kisspeptin neurons respond to sex steroid feedback, including testosterone and oestradiol-related signaling.[6][10] In simplified terms, these neurons help the brain sense reproductive hormone status and adjust GnRH output.
This feedback system is one reason kisspeptin may affect LH secretion in men and women differently across physiologic states. Menstrual cycle phase, menopause status, hypogonadism, metabolic disease, and sex steroid therapy can all affect interpretation of a response to kisspeptin.[4][6]14
What Is Kisspeptin Peptide Used For or Studied For?
Kisspeptin peptide is studied mainly for reproductive endocrine questions. It is not an FDA-approved fertility drug, testosterone therapy, libido drug, or puberty treatment in routine clinical use.[8][9]
The most clinically relevant research areas include assisted reproduction, ovulation triggering, hypothalamic amenorrhea, hypogonadotropic hypogonadism, male reproductive hormone secretion, and brain responses related to sexual and emotional processing.[5][7]15
Fertility, Ovulation Triggering, and Assisted Reproduction Research
One major research area is whether kisspeptin can trigger oocyte maturation during in vitro fertilization while potentially reducing ovarian hyperstimulation risk in selected populations.[5][7] Studies from UK research groups, including work associated with Imperial College London and Hammersmith Hospital, have explored kisspeptin-54 in assisted reproduction settings.[5][7]
These findings are promising in a research context, but they do not mean kisspeptin is a general fertility treatment. Assisted reproduction studies involve careful patient selection, ovarian monitoring, laboratory procedures, and clinician oversight.[5][7]
Hypogonadotropic Hypogonadism and Other Reproductive Disorders
Because KISS1R mutations can cause hypogonadotropic hypogonadism, researchers have examined whether kisspeptin administration can help probe or stimulate the reproductive axis.[11][12] This is different from proving that kisspeptin is an approved treatment for all forms of hypogonadism or infertility.
Some studies have also investigated kisspeptin responses in men with type 2 diabetes or other metabolic contexts, because metabolism can interact with reproductive hormone signaling.16 Such studies remain specialized and should not be generalized to personal testosterone production claims.
Libido, Mood, and Sexual Function Studies
Kisspeptin has been studied for effects on brain responses to sexual and emotional stimuli in humans.17 This research is relevant to libido, mood, and hypoactive sexual desire disorder hypotheses, but it remains early human evidence.
Brain-imaging or hormone-response findings do not prove that kisspeptin improves sexual dysfunction as a routine therapy. Sexual function is complex and can involve endocrine, vascular, neurologic, psychological, medication-related, and relationship factors.[17]
Potential Benefits of Kisspeptin Peptide: What Evidence Supports Them?
Potential benefits of kisspeptin are best organized by evidence level. The strongest mechanistic support is for stimulation of GnRH-related signaling, LH release, and reproductive axis activation.[6][10] The most clinically relevant human evidence is in controlled endocrine studies and assisted reproduction research.[4][5][7]
Claims about broad testosterone enhancement, fertility improvement, libido improvement, anti-aging, mood benefits, or metabolic effects need more caution. Some have early human or mechanistic support, while others remain unsupported online claims.[16][17]
| Evidence Area | What Has Been Studied | Evidence Level | What It Can and Cannot Show |
|---|---|---|---|
| GnRH, LH, and FSH signaling | Kisspeptin receptor activation and downstream gonadotropin release.[6][10] | Clinical / mechanistic | Supports reproductive axis biology; does not prove broad therapeutic benefit. |
| Assisted reproduction | Kisspeptin-54 as an oocyte maturation trigger in IVF research.[5][7] | Early human / clinical | Suggests possible fertility-protocol utility; not a general fertility recommendation. |
| Male reproductive hormones | LH secretion and testosterone-related endpoints in controlled studies.[4][14] | Early human | Shows endocrine responses; does not establish testosterone therapy. |
| Libido and brain processing | Neuroimaging and psychosexual-response research.[17] | Early human | Generates hypotheses; does not prove treatment for sexual dysfunction. |
| Cancer/metastasis biology | KISS1 was identified in metastasis-suppression research.18 | Preclinical / translational | Explains historical biology; not evidence for peptide cancer treatment. |
Benefits of Kisspeptin for Luteinizing Hormone and FSH Signaling
Human studies have shown that kisspeptin administration can increase LH secretion in controlled settings.[4][14] Because LH and FSH are downstream of GnRH, these hormone changes are central to the proposed therapeutic role of kisspeptin in reproduction.[6]
The limitation is that hormone release is an intermediate endpoint. It may be useful in research, but it is not the same as pregnancy, restored fertility, sustained testosterone normalization, or symptom improvement.[5][6]
Effects of Kisspeptin on Testosterone Levels in Studied Settings
In men, kisspeptin-related increases in LH may lead to changes in serum testosterone, depending on baseline physiology and study design.[4][14] Some research has measured serum testosterone and LH secretion after kisspeptin exposure.
However, kisspeptin should not be described as a testosterone replacement therapy. Testosterone levels are regulated by multiple factors, and treating hypogonadism requires diagnosis, monitoring, risk assessment, and approved therapeutic options when appropriate.[11][16]
Human Research on Kisspeptin and Kisspeptin-10
Human research supports a real biological response to kisspeptin, especially in reproductive hormone secretion. Studies have evaluated kisspeptin-10 and kisspeptin-54 in healthy men, women, infertility settings, and specialized endocrine populations.[4][5][7][14]
The overall evidence base remains limited by small samples, specialized settings, short follow-up, and variation in peptide form, route, and endpoints. These are not weaknesses of the science so much as signs that kisspeptin is still largely an investigational research tool.[9]
Early Clinical Trials in Healthy Men and Women
Early human studies in healthy men demonstrated that kisspeptin-54 could stimulate the hypothalamic-pituitary-gonadal axis.[4] Later studies examined kisspeptin-10 effects on LH pulse frequency and reproductive hormone secretion.[14]
Women’s studies have shown that response can vary with menstrual cycle phase and reproductive state.[6][10] This matters because the same peptide may produce different hormone patterns depending on ovarian steroid feedback and hypothalamic sensitivity.
Administration of Kisspeptin-10 in Assisted Fertility Settings
Most assisted fertility research has focused on kisspeptin-54 rather than kisspeptin-10, especially for triggering oocyte maturation in IVF protocols.[5][7] Kisspeptin-10 has been widely studied in endocrine physiology, but fertility-protocol evidence should be interpreted by the exact peptide used.
Administration of kisspeptin-10 or kisspeptin-54 in studies occurs under research or clinical supervision. These protocols include screening, monitoring, and adverse-event tracking that are not present in unregulated self-use settings.[5][7][9]
Research From Imperial College London and Hammersmith Hospital
Several prominent human kisspeptin studies have come from UK academic groups, including Imperial College London and Hammersmith Hospital research networks.[5][7][17] These studies helped define kisspeptin as a serious reproductive endocrinology research topic.
Their results should still be interpreted within study boundaries. A positive endocrine or IVF endpoint in a monitored trial does not establish broad over-the-counter therapeutic use.[5][7]
Preclinical Evidence and Mechanistic Research
Preclinical evidence has shaped much of what is known about kisspeptin signaling. Animal and cellular studies helped identify how kisspeptin neurons, KISS1R, GnRH neurons, and sex steroid feedback interact.[6][10]
Preclinical findings are valuable for mechanism, but they cannot prove human safety or effectiveness. Translation from animal models to human reproductive medicine requires carefully designed clinical studies.[6][10]
Animal Models of Kisspeptin in Reproduction
Animal models show that kisspeptin signaling is essential for normal reproductive function. Disruption of kisspeptin or KISS1R signaling can impair puberty and fertility-related endpoints in model systems.[6][10]
These findings align with human genetic data linking receptor defects to hypogonadotropic hypogonadism.[11][12] Together, they support the role of kisspeptin in reproduction, but they do not define a general therapeutic protocol.
Kisspeptin Expression, Metastasis, and Cancer Biology Context
The KISS1 gene was first discussed in cancer biology because of metastasis-suppression research.[18] Later work identified KISS1-derived peptides as ligands for a G protein-coupled receptor, connecting metastasis biology and endocrine signaling.[2][3]
This history can be confusing. It does not mean kisspeptin peptide is a cancer treatment. Cancer-related findings are largely mechanistic and translational, and any oncology claim would require separate clinical evidence.[18]
Evidence Limitations and Unsupported Online Claims
The evidence for kisspeptin is strongest for reproductive axis biology and controlled hormone responses. It is weaker for broad online claims about testosterone optimization, libido, anti-aging, mood, metabolism, or generalized fertility enhancement.[6][16][17]
Unsupported claims often skip the difference between a measurable hormone change and a meaningful clinical outcome. Responsible interpretation requires asking what was studied, in whom, by what route, for how long, and with what endpoint.
What Clinical Evidence Can and Cannot Prove Today
Current human evidence can show that kisspeptin can stimulate reproductive hormone release under certain conditions.[4][14] It can also show that kisspeptin-54 has been studied as an oocyte maturation trigger in IVF research.[5][7]
It cannot yet prove that kisspeptin is safe or effective for unsupervised fertility treatment, testosterone enhancement, puberty disorders, sexual dysfunction, or long-term endocrine therapy. Those questions require larger trials, longer follow-up, and regulatory review.[8][9]
Source Quality Filter for Kisspeptin Research
A useful source-quality filter starts with regulatory databases, ClinicalTrials.gov, PubMed-indexed studies, systematic reviews, and academic medical centers.[8][9] Lower-quality sources include peptide vendor pages, clinic marketing pages, forums, bodybuilding content, and unsourced social media claims.
When reading about kisspeptin, the strongest questions are: Was this a human study? Was it randomized or controlled? Which peptide was used? What route and dose were used? Were adverse events reported? Was the outcome clinical or only hormonal?
Side Effects of Kisspeptin Peptide Reported in Studies
Published kisspeptin studies generally report safety within monitored research contexts, but that is not the same as proving safety for long-term or unsupervised use.[5][7] Reported and monitored issues may include injection-site reactions, headache, nausea, abdominal symptoms, hormone-related symptoms, ovarian response in fertility protocols, and laboratory changes, depending on study design.[5][7]
Because kisspeptin affects reproductive hormone signaling, side effects should be considered endocrine-relevant even when short-term tolerability appears acceptable. Long-term effects, repeated exposure, and use in people with reproductive disorders remain less certain.[6][9]
Commonly Monitored Adverse Events After Kisspeptin Administration
Clinical studies commonly monitor vital signs, symptoms, hormone levels, ovarian response, and adverse events after kisspeptin administration.[5][7] In assisted reproduction research, monitoring also includes ovarian stimulation context and risk of ovarian hyperstimulation syndrome.[7]
Safety findings from supervised trials should not be extrapolated to compounded or unapproved products. Product purity, identity, sterility, dose accuracy, and storage conditions can differ outside regulated clinical settings.19
Hormone-Related Symptoms and Menstrual Cycle Considerations
Because kisspeptin can influence LH and FSH signaling, hormone-related symptoms are biologically plausible. These may be especially relevant in people with menstrual irregularity, polycystic ovary syndrome, hypothalamic amenorrhea, infertility, menopause, or sex steroid therapy exposure.[6][10]
Menstrual cycle timing can also affect response to kisspeptin. A result from one cycle phase or clinical population may not apply to another.[6]
Safety Considerations, Contraindications, and Monitoring
There is no broad approved-label contraindication list for kisspeptin because there is no FDA-approved routine therapeutic kisspeptin product.[8] Safety considerations therefore come from study exclusions, reproductive endocrinology principles, and general caution around investigational peptides.[5][7][19]
People with endocrine disorders, hormone-sensitive conditions, infertility diagnoses, pituitary disease, hypothalamic disease, or reproductive cancers require clinician-guided evaluation. The same is true for anyone using GnRH analogs, gonadotropins, testosterone, estradiol, contraceptives, or fertility medications.[6][19]
Pregnancy, Breastfeeding, Puberty Disorders, and Endocrine Disease Caution
Pregnancy, breastfeeding, childhood puberty disorders, precocious puberty, hypogonadotropic hypogonadism, and infertility are high-risk medical contexts. Kisspeptin signaling is directly tied to reproductive hormone biology, so these situations should not be approached through self-treatment.[6][11][12]
Published research does not establish kisspeptin as safe for pregnancy, breastfeeding, pediatric self-use, or unsupervised endocrine disease management. These areas require specialist oversight and, where applicable, approved therapies.[8][9]
Why Medical Supervision Matters for Reproductive Hormone Therapy
Medical supervision matters because LH, FSH, testosterone, estradiol, progesterone, prolactin, thyroid function, metabolic status, and pituitary function can all affect reproductive symptoms. A peptide that changes one hormone signal can have downstream effects across the endocrine system.[6][10]
Clinician oversight also helps distinguish causes of infertility, amenorrhea, low libido, low testosterone, or delayed puberty. These symptoms can have many causes, and treating the wrong mechanism can delay appropriate care.[11][12]
Biomarkers Clinicians May Monitor in Research or Care
Research protocols may measure LH, FSH, estradiol, progesterone, testosterone, gonadotropin pulses, ovulation markers, ultrasound findings, and adverse events.[4][5][7][14] In fertility settings, ovarian response and oocyte maturation endpoints may also be tracked.[5][7]
These biomarkers are not do-it-yourself targets. They require medical interpretation because normal ranges and clinical meaning depend on sex, age, cycle phase, medications, diagnosis, and reproductive goals.[6]
Drug Interactions and Hormone Therapy Considerations
Formal drug interaction data for kisspeptin are limited because it is not an approved routine medication with a full prescribing label.[8] The main concern is pharmacodynamic interaction with therapies that act on the reproductive axis.
This includes GnRH analogs, gonadotropins, human chorionic gonadotropin, fertility medications, testosterone therapy, estradiol therapy, contraceptives, anti-androgens, and other endocrine drugs. Combining hormone-active interventions can change clinical interpretation and risk.[6][19]
Interactions With GnRH Analogs, Gonadotropins, and Sex Steroids
GnRH analogs, gonadotropins, and sex steroids act within the same reproductive axis that kisspeptin influences.[6] That overlap creates a plausible interaction concern even when formal interaction trials are lacking.
In assisted reproduction, medications are timed carefully to control follicle development, ovulation triggering, and luteal support. Adding an investigational peptide outside a protocol could disrupt that timing and safety monitoring.[5][7]
Considerations for Testosterone and Oestradiol Therapies
Testosterone and oestradiol therapies can alter feedback signals to the hypothalamus and pituitary.[6] Because kisspeptin neurons respond to sex steroid feedback, concurrent hormone therapy may change the response to kisspeptin.
This is especially relevant for people using testosterone replacement therapy, feminizing hormone therapy, fertility preservation regimens, or gender-affirming hormone therapy. Evidence is not sufficient to provide generalized interaction rules, so clinician review is essential.[6][19]
Dosage Information From Published Kisspeptin Studies
Dosage information for kisspeptin should be read as research context only. Published studies have used supervised protocols with kisspeptin-10 or kisspeptin-54, including intravenous bolus, intravenous infusion, and subcutaneous administration in specific populations.[4][5][7][14]
Study doses should not be interpreted as personal dosing advice. The meaning of a dose depends on peptide form, route, purity, formulation, body-weight scaling, monitoring, endpoint, and exclusion criteria.[4][5]
Why There Is No Approved Label Dose for Routine Kisspeptin Therapy
There is no FDA-approved label dose for routine kisspeptin therapy because kisspeptin is not listed as an approved drug product for general therapeutic use in the FDA Drugs@FDA database.[8] That means there is no regulator-reviewed prescribing information defining indications, dosing, contraindications, warnings, adverse reactions, and manufacturing standards for routine use.[8]
Clinical trial protocols are not substitutes for prescribing labels. They are designed for specific research questions and include safeguards that may not exist outside a trial.[9]
How Study Doses Differ From Personal Medical Advice
Published kisspeptin studies may report doses in research units such as nmol/kg or infusion rates, not consumer-style protocols.[4][5][14] Those doses were selected for defined study populations and endpoints.
A research dose is not a recommendation. Personal medical decisions require diagnosis, approved alternatives, risk assessment, product quality verification, and clinician supervision.[8][19]
Administration Routes Discussed in Medical Literature
Administration routes discussed in the literature include intravenous injection, intravenous infusion, and subcutaneous injection in controlled settings.[4][5][7][14] Route matters because it affects peak concentration, duration of receptor stimulation, and hormone-response interpretation.
This article does not provide injection instructions, reconstitution steps, storage guidance, or self-administration protocols. Administration details in studies are for interpreting evidence, not guiding personal use.[4][5]
Intravenous, Subcutaneous, and Infusion Contexts in Trials
Intravenous studies are often used to assess acute endocrine responses, such as LH release or pulse frequency.[4][14] Subcutaneous kisspeptin-54 has been studied in assisted reproduction protocols because it can be integrated into monitored fertility treatment workflows.[5][7]
Infusion studies may help researchers understand dose-response and hormone dynamics. These settings involve trained staff, clinical monitoring, and protocol oversight.[4]
Why This Is Not an Injection Protocol
An injection protocol would require patient-specific diagnosis, sterile product standards, route selection, dose selection, monitoring, adverse-event planning, and legal prescribing context. None of that can be replaced by an informational article.[8][19]
Unapproved or compounded peptides may also raise quality concerns, including identity, potency, sterility, and contamination risks. FDA materials on compounding emphasize that compounded drugs are not FDA-approved in the same way as approved products.[19]
Is Kisspeptin Peptide FDA-Approved or Legally Available?
Kisspeptin peptide does not have an FDA-approved routine therapeutic indication listed in Drugs@FDA.[8] ClinicalTrials.gov lists kisspeptin-related studies, which supports its investigational research status rather than broad approved medical use.[9]
Legal status can vary by country and product type. Regulatory status matters because approved products are reviewed for specific indications, dosing, labeling, manufacturing quality, and safety information.[8][19]
Investigational Status and Clinical Trial Context
Kisspeptin has been studied in clinical trials for reproductive hormone and fertility-related questions.[9] Trial participation is different from commercial availability because trials use protocols, oversight, eligibility criteria, and adverse-event reporting.
Readers should be cautious when online sources imply that research peptides are equivalent to approved medicines. Investigational evidence does not establish legal, safe, or effective personal use.[8][19]
Why Unapproved or Compounded Peptides Require Caution
Compounded drugs can be appropriate in certain medical contexts, but they are not FDA-approved and do not undergo the same premarket review for safety, effectiveness, and manufacturing quality.[19] This distinction is especially important for peptides, where small changes in sequence, purity, or formulation can affect biological activity.
Unapproved peptide marketing often relies on mechanistic claims, animal findings, or testimonials. Those claims should be weighed against the absence of approved labeling, long-term safety data, and consistent product-quality oversight.[8][19]
How Kisspeptin Compares With Related Reproductive Hormone Therapies
Kisspeptin acts upstream of GnRH, while many established reproductive therapies act downstream or replace specific hormones. For example, GnRH analogs act at the pituitary level, gonadotropins provide LH/FSH-like stimulation, hCG can mimic LH activity, and sex steroid therapies replace or modify downstream hormone exposure.[6]
The key comparison is not “which is best,” but what evidence and regulatory status support each option. Approved therapies have labeling for defined indications, while kisspeptin remains mainly a research tool in most settings.[8][9]
Key Questions to Discuss With a Clinician Before Considering Hormone Research Claims
Use this checklist to keep the conversation evidence-focused:
- What diagnosis or symptom is being evaluated: infertility, amenorrhea, low testosterone, delayed puberty, libido, or another issue?
- Is there an approved therapy with established dosing, monitoring, and safety information?
- Is the kisspeptin claim based on human outcomes, hormone biomarkers, animal data, or online anecdotes?
- Which peptide was studied: kisspeptin-10, kisspeptin-54, or another fragment?
- What route and monitoring were used in the study?
- Are pregnancy, breastfeeding, puberty, pituitary disease, cancer history, or hormone-sensitive conditions relevant?
- Could current medications, testosterone, oestradiol, contraceptives, GnRH analogs, gonadotropins, or fertility drugs interact with the reproductive axis?
- What adverse events and long-term uncertainties remain?
The safest way to interpret kisspeptin peptide is through evidence quality, regulatory status, safety data, and clinician-guided decision-making. Strong conclusions require approved labeling or well-designed human studies; weaker claims should be treated cautiously.
REFERENCES
- National Center for Biotechnology Information. PubChem Compound Summary: Kisspeptin-10. PubChem. Accessed 2026.
- Ohtaki T, Shintani Y, Honda S, et al. Metastasis suppressor gene KiSS-1 encodes peptide ligand of a G-protein-coupled receptor. Nature. 2001.
- Kotani M, Detheux M, Vandenbogaerde A, et al. The metastasis suppressor gene KiSS-1 encodes kisspeptins, the natural ligands of the orphan G protein-coupled receptor GPR54. Journal of Biological Chemistry. 2001.
- Dhillo WS, Chaudhri OB, Patterson M, et al. Kisspeptin-54 stimulates the hypothalamic-pituitary gonadal axis in human males. Journal of Clinical Endocrinology & Metabolism. 2005.
- Jayasena CN, Abbara A, Comninos AN, et al. Kisspeptin-54 triggers egg maturation in women undergoing in vitro fertilization. Journal of Clinical Investigation. 2014.
- Oakley AE, Clifton DK, Steiner RA. Kisspeptin signaling in the brain. Endocrine Reviews. 2009.
- Abbara A, Jayasena CN, Christopoulos G, et al. Efficacy of kisspeptin-54 to trigger oocyte maturation in women at high risk of ovarian hyperstimulation syndrome. Journal of Clinical Endocrinology & Metabolism. 2015.
- U.S. Food and Drug Administration. Drugs@FDA: FDA-Approved Drugs Database. FDA official database. Accessed 2026.
- U.S. National Library of Medicine. ClinicalTrials.gov search results for kisspeptin. ClinicalTrials.gov. Accessed 2026.
- Pinilla L, Aguilar E, Dieguez C, Millar RP, Tena-Sempere M. Kisspeptins and reproduction: physiological roles and regulatory mechanisms. Physiological Reviews. 2012.
- Seminara SB, Messager S, Chatzidaki EE, et al. The GPR54 gene as a regulator of puberty. New England Journal of Medicine. 2003.
- de Roux N, Genin E, Carel JC, Matsuda F, Chaussain JL, Milgrom E. Hypogonadotropic hypogonadism due to loss of function of the KiSS1-derived peptide receptor GPR54. Proceedings of the National Academy of Sciences. 2003.
- PubMed / National Library of Medicine. Kisspeptin and precocious puberty literature search. PubMed database. Accessed 2026.
- PubMed / National Library of Medicine. Kisspeptin-10, LH pulse frequency, and male reproductive hormone studies. PubMed database. Accessed 2026.
- PubMed / National Library of Medicine. Kisspeptin and hypothalamic amenorrhea clinical trial literature. PubMed database. Accessed 2026.
- PubMed / National Library of Medicine. Kisspeptin, men with type 2 diabetes, LH, and testosterone literature. PubMed database. Accessed 2026.
- PubMed / National Library of Medicine. Kisspeptin, sexual and emotional brain processing in humans literature. PubMed database. Accessed 2026.
- Lee JH, Miele ME, Hicks DJ, et al. KiSS-1, a novel human malignant melanoma metastasis-suppressor gene. Journal of the National Cancer Institute. 1996.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers. FDA official information. Accessed 2026.
Contributing Authors
The following authors are recognized for published research that helped shape the scientific and clinical context discussed in this article.
Waljit S. Dhillo
Author profile: Imperial College London Profile
Waljit S. Dhillo is an author of clinical research relevant to kisspeptin peptide physiology, reproductive endocrinology, and the hypothalamic-pituitary-gonadal axis. His published work is useful for understanding how kisspeptin has been studied in controlled human settings, including hormone-response studies and assisted reproduction research. These publications help frame the distinction between biologically plausible mechanism of action, early clinical evidence, and the evidence limitations that remain when interpreting investigational peptide research.
Selected publications:
- Kisspeptin-54 stimulates the hypothalamic-pituitary gonadal axis in human males — Journal of Clinical Endocrinology & Metabolism, 2005. DOI: 10.1210/jc.2005-1468
- Kisspeptin-54 triggers egg maturation in women undergoing in vitro fertilization — Journal of Clinical Investigation, 2014. PMID: 24569457
Channa N. Jayasena
Author profile: Imperial College London Profile
Channa N. Jayasena is an author of human clinical studies examining kisspeptin in reproductive hormone and assisted fertility research. His publications are relevant to the clinical evidence discussed in this article because they evaluate kisspeptin-54 in medically supervised fertility settings, including oocyte maturation and ovarian hyperstimulation risk contexts. This work provides useful background for interpreting kisspeptin as an investigational reproductive hormone signal rather than as a broadly established therapeutic product.
Selected publications:
- Kisspeptin-54 triggers egg maturation in women undergoing in vitro fertilization — Journal of Clinical Investigation, 2014. PMID: 24569457
- Efficacy of kisspeptin-54 to trigger oocyte maturation in women at high risk of ovarian hyperstimulation syndrome — Journal of Clinical Endocrinology & Metabolism, 2015. PMID: 26079790